

Clinical characteristics of phenotypes of fecal incontinence
- PMID: 36967451
- PMCID: PMC10169873
- DOI: 10.1007/s10151-023-02778-2
Clinical characteristics of phenotypes of fecal incontinence
Abstract
Purpose: Fecal incontinence (FI) is common, but its etiology is complex with large knowledge gaps. Several phenotypes of FI are known, but the phenotype is often not decisive in the chosen therapy. In this study we aimed to assess the association of the clinical characteristics of patients with FI and the various phenotypes, in order to establish a targeted clinical treatment decision tree.
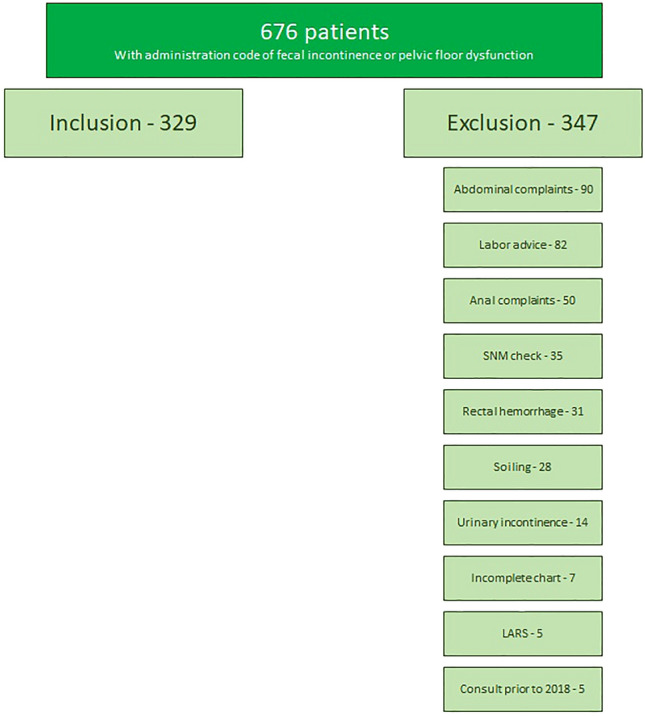
Methods: We retrospectively studied the charts of patients with FI, who visited our institute from January 2018 until December 2020. Patients were divided into the following groups: passive fecal loss, urge incontinence, combined fecal incontinence with predominantly passive fecal loss, and combined fecal incontinence with predominantly urge incontinence. We compared the characteristics between the passive and urge incontinence groups, the passive and combined mainly passive groups, and the urge and combined mainly urge groups.
Results: Patients with passive incintinence were older, more often had a flaccid anus with presence of a mucosal prolapse, and had a lower resting pressure on anorectal manometry. Patients with urge incontinence were younger and more often had a history of birth trauma. The combined groups showed characteristics of both of the main types of FI.
Conclusion: Differentiating into phenotypes of FI can be clinically meaningful. The patient history and clinical judgement of the consulting specialist, rather than the physical characteristics, seem to be decisive in the categorization. Additional diagnostic testing can be helpful in complicated cases, but should not be used routinely.
Keywords: Fecal incontinence; Phenotypes; Proctology; Surgery.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
References
-
- Bharucha AE, Dunivan G, Goode PS, et al. Epidemiology, pathophysiology, and classification of fecal incontinence: state of the science summary for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) workshop. Am J Gastroenterol. 2015;110(1):127–136. doi: 10.1038/ajg.2014.396. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
