

The therapeutic potential of targeting minimal residual disease in melanoma
- PMID: 36967556
- PMCID: PMC10040726
- DOI: 10.1002/ctm2.1197
The therapeutic potential of targeting minimal residual disease in melanoma
Abstract
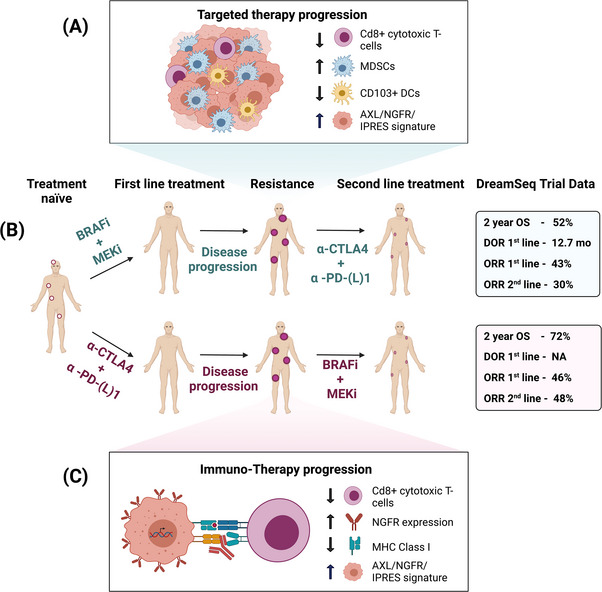
Background: Cutaneous melanoma is a lethal form of skin cancer with morbidity and mortality rates highest amongst European, North American and Australasian populations. The developments of targeted therapies (TTs) directed at the oncogene BRAF and its downstream mediator MEK, and immune checkpoint inhibitors (ICI), have revolutionized the treatment of metastatic melanoma, improving patient outcomes. However, both TT and ICI have their limitations. Although TTs are associated with high initial response rates, these are typically short-lived due to resistance. Conversely, although ICIs provide more durable responses, they have lower initial response rates. Due to these distinct yet complementary response profiles, it has been proposed that sequencing ICI with TT could lead to a high frequency of durable responses whilst circumventing the toxicity associated with combined ICI + TT treatment. However, several questions remain unanswered, including the mechanisms underpinning this synergy and the optimal sequencing strategy. The key to determining this is to uncover the biology of each phase of the therapeutic response.
Aims and methods: In this review, we show that melanoma responds to TT and ICI in three phases: early response, minimal residual disease (MRD) and disease progression. We explore the effects of ICI and TT on melanoma cells and the tumour immune microenvironment, with a particular focus on MRD which is predicted to underpin the development of acquired resistance in the third phase of response.
Conclusion: In doing so, we provide a new framework which may inform novel therapeutic approaches for melanoma, including optimal sequencing strategies and agents that target MRD, thereby ultimately improving clinical outcomes for patients.
Keywords: BRAF/MEK inhibitors; acquired resistance; combination treatment; cross-resistance; immune checkpoint inhibitors; intrinsic resistance; melanoma; minimal residual disease.
© 2023 The Authors. Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
There are no conflicts of interest to disclose.
Figures


References
-
- Ferlay J, Ervik M, Lam F, et al. Global cancer observatory. Cancer today; 2020;1‐6.
-
- Robert C, Grob JJ, Stroyakovskiy D, et al. Five‐year outcomes with dabrafenib plus trametinib in metastatic melanoma. N Engl J Med. 2019;381(7):626‐636. - PubMed
-
- Larkin J, Chiarion‐Sileni V, Gonzalez R, et al. Five‐year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381(16):1535‐1546. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials