

Clinical and endoscopic characteristics of sessile serrated lesions with dysplasia/carcinoma
- PMID: 36967594
- PMCID: PMC10175875
- DOI: 10.3904/kjim.2022.322
Clinical and endoscopic characteristics of sessile serrated lesions with dysplasia/carcinoma
Abstract
Background/aims: Some sessile serrated lesions (SSLs) progress into dysplasia and colorectal cancer, however, the clinical and endoscopic characteristics of SSLs with dysplasia remain to be determined. In this study, we elucidated these characteristics in SSLs with dysplasia/carcinoma, compared with those of SSLs without dysplasia.
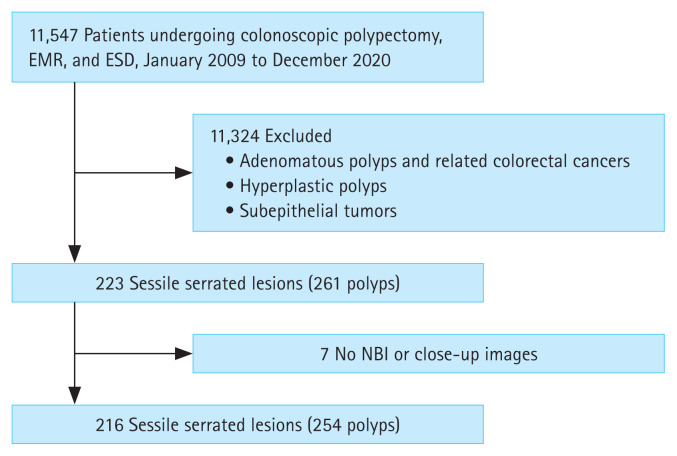
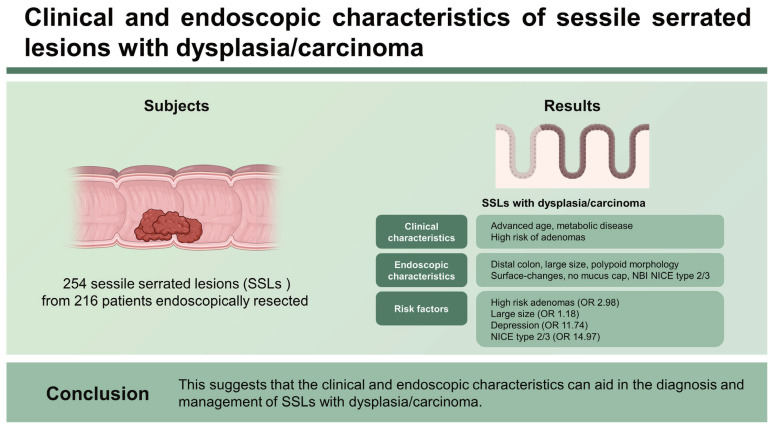
Methods: We retrospectively collected the clinical, endoscopic, and pathological data of 254 SSLs from 216 patients endoscopically resected between January 2009 and December 2020.
Results: All SSLs included 179 without dysplasia and 75 with dysplasia/carcinoma, including 55 with low-grade dysplasia, 10 with high-grade dysplasia, and 10 with submucosal cancer. In clinical characteristics, SSLs with dysplasia/carcinoma were significantly associated with advanced age, metabolic diseases, and high-risk adenomas. In endoscopic characteristics, SSLs with dysplasia/carcinoma were significantly associated with the distal colon, large size, polypoid morphology, surface-changes, no mucus cap, and narrow-band imaging international colorectal endoscopic classification (NICE) type 2/3. In the multivariate analysis, high-risk adenomas (odds ratio [OR], 2.98; p = 0.01), large size (OR, 1.18; p < 0.01), depression (OR, 11.74; p = 0.03), and NICE type 2/3 (OR, 14.97; p < 0.01) were significantly associated with SSLs with dysplasia/carcinoma.
Conclusion: SSLs had a higher risk of dysplasia in the distal colon than in the proximal colon. SSLs with large size, depression, and adenomatous surface-patterns, as well as those in patients with high-risk adenomas, increased the risk of dysplasia/ carcinoma. This suggests that the clinical and endoscopic characteristics can aid in the diagnosis and management of SSLs with dysplasia/carcinoma.
Keywords: Carcinoma; Clinical and endoscopic characteristics; Dysplasia; Sessile serrated lesions.
Conflict of interest statement
The authors disclose no conflicts.
Figures
References
-
- Torlakovic E, Skovlund E, Snover DC, Torlakovic G, Nesland JM. Morphologic reappraisal of serrated colorectal polyps. Am J Surg Pathol. 2003;27:65–81. - PubMed
-
- Carr NJ, Mahajan H, Tan KL, Hawkins NJ, Ward RL. Serrated and non-serrated polyps of the colorectum: their prevalence in an unselected case series and correlation of BRAF mutation analysis with the diagnosis of sessile serrated adenoma. J Clin Pathol. 2009;62:516–518. - PubMed
-
- Lash RH, Genta RM, Schuler CM. Sessile serrated adenomas: prevalence of dysplasia and carcinoma in 2139 patients. J Clin Pathol. 2010;63:681–686. - PubMed
-
- East JE, Vieth M, Rex DK. Serrated lesions in colorectal cancer screening: detection, resection, pathology and surveillance. Gut. 2015;64:991–1000. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous