

Open versus percutaneous tube thoracostomy with and without thoracic lavage for traumatic hemothorax: a novel randomized controlled simulation trial
- PMID: 36967862
- PMCID: PMC10030794
- DOI: 10.1136/tsaco-2022-001050
Open versus percutaneous tube thoracostomy with and without thoracic lavage for traumatic hemothorax: a novel randomized controlled simulation trial
Abstract
Objective: To quantify and assess the relative performance parameters of thoracic lavage and percutaneous thoracostomy (PT) using a novel, basic science 2×2 randomized controlled simulation trial.
Summary background data: Treatment of traumatic hemothorax (HTX) with open tube thoracostomy (TT) is painful and retained HTX is common. PT is potentially less painful whereas thoracic lavage may reduce retained HTX. Yet, procedural time and the feasibility of combining PT with lavage remain undefined.
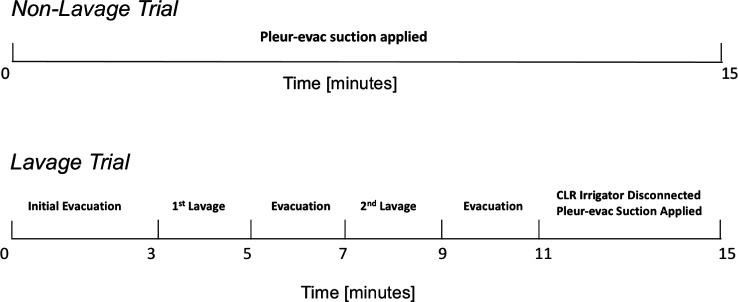
Methods: A simulated partially clotted HTX (2%-gelatin-saline mixture) was loaded into a TT trainer and then evacuated after randomization to one of four protocols: TT+/-lavage or PT+/-lavage. Standardized inserts with fixed 28-Fr TT or 14-Fr PT positioning were used to minimize tube positioning variability. Lavage consisted of two 500 mL aliquots of warm saline after initial HTX evacuation. The primary outcome was HTX volume evacuated. The secondary outcome was additional procedural time required for the addition of the lavage.
Results: A total of 40 simulated HTX trials were randomized. TT alone evacuated a median of 1236 mL (IQR 1168, 1294) leaving a residual volume of 265 mL (IQR 206, 333). PT alone resulted in a significantly greater median residual volume of 588 mL (IQR 497, 646) (p=0.002). Adding lavage resulted in similar residual volumes for TT compared with TT alone but significantly less for PT compared with PT alone (p=0.002). Lavage increased procedural time for TT by a median of 7.0 min (IQR 6.5, 8.0) vs 11.7 min (IQR 10.2, 12.0) for PT (p<0.001).
Conclusion: This simulation trial characterized HTX evacuation in a standardized fashion. Adding lavage to thoracostomy placement may improve evacuation, particularly for small-diameter tubes, with little added procedural time. Further prospective clinical study is warranted.
Level of evidence: NA.
Keywords: Hemothorax; Thoracic Injuries.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ANS is Chief Medical Officer of CLR Medical which makes the CLR irrigator. The remaining authors declare no conflict of interest. This work was made possible through the generous support of the Measey Scholars Program, Department of Surgery, Perelman School of Medicine at the University of Pennsylvania. CLR Medical provided CLR Irrigators in-kind but did not provide study funding and had no role in the study design or data analysis.
Figures



References
-
- Mancini MC. Hemothorax [Internet]. In: Milliken JC, ed. Medscape. 2006. Available: https://emedicine.medscape.com/article/2047916-overview
-
- Ivey KM, White CE, Wallum TE, Aden JK, Cannon JW, Chung KK, McNeil JD, Cohn SM, Blackbourne LH. Thoracic injuries in US combat casualties: a 10-year review of operation enduring freedom and iraqi freedom. J Trauma Acute Care Surg 2012;73:S514–9. - PubMed
-
- Patel NJ, Dultz L, Ladhani HA, Cullinane DC, Klein E, McNickle AG, Bugaev N, Fraser DR, Kartiko S, Dodgion C, et al. Management of simple and retained hemothorax: A practice management guideline from the eastern association for the surgery of trauma. Am J Surg 2021;221:873–84. 10.1016/j.amjsurg.2020.11.032 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials