

Multiregional Sequencing Analysis Reveals Extensive Genetic Heterogeneity in Gastric Tumors from Latinos
- PMID: 36970058
- PMCID: PMC10035402
- DOI: 10.1158/2767-9764.CRC-22-0149
Multiregional Sequencing Analysis Reveals Extensive Genetic Heterogeneity in Gastric Tumors from Latinos
Abstract
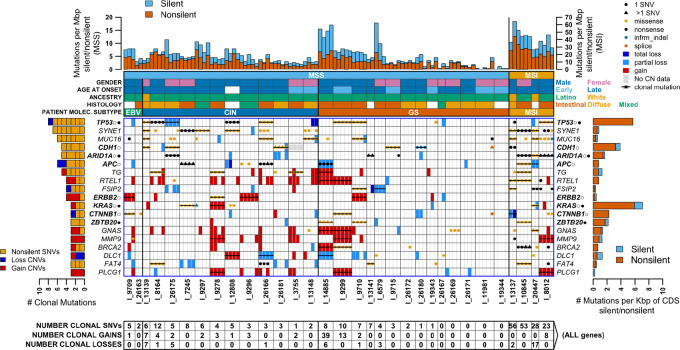
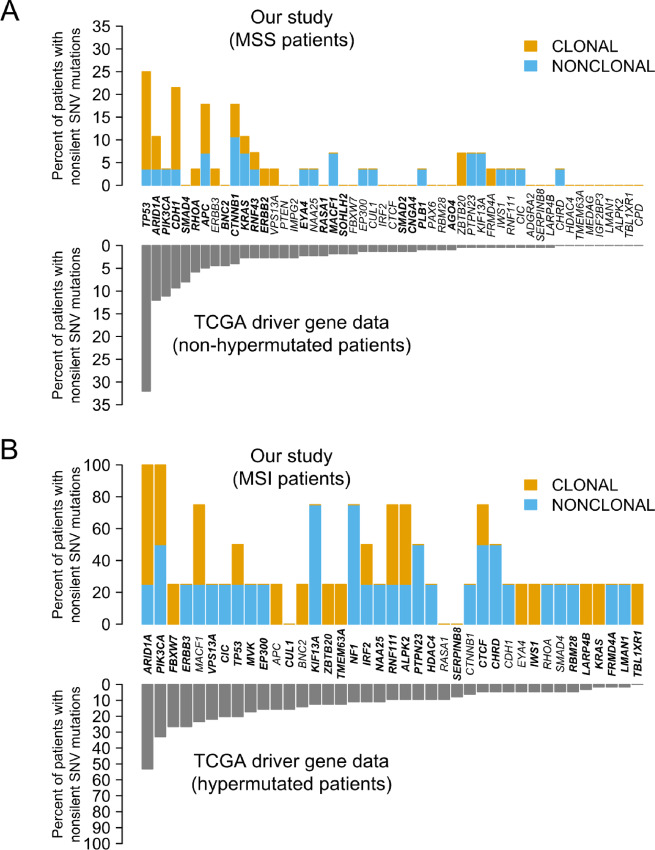
Gastric cancer is a leading cause of cancer mortality and health disparities in Latinos. We evaluated gastric intratumoral heterogeneity using multiregional sequencing of >700 cancer genes in 115 tumor biopsies from 32 patients, 29 who were Latinos. Analyses focused on comparisons with The Cancer Genome Atlas (TCGA) and on mutation clonality, druggability, and signatures. We found that only approximately 30% of all mutations were clonal and that only 61% of the known TCGA gastric cancer drivers harbored clonal mutations. Multiple clonal mutations were found in new candidate gastric cancer drivers such as EYS, FAT4, PCDHA1, RAD50, EXO1, RECQL4, and FSIP2. The genomically stable (GS) molecular subtype, which has the worse prognosis, was identified in 48% of our Latino patients, a fraction that was >2.3-fold higher than in TCGA Asian and White patients. Only a third of all tumors harbored clonal pathogenic mutations in druggable genes, with most (93%) GS tumors lacking actionable clonal mutations. Mutation signature analyses revealed that, in microsatellite-stable (MSS) tumors, DNA repair mutations were common for both tumor initiation and progression, while tobacco, POLE, and inflammation signatures likely initiate carcinogenesis. MSS tumor progression was likely driven by aging- and aflatoxin-associated mutations, as these latter changes were usually nonclonal. In microsatellite-unstable tumors, nonclonal tobacco-associated mutations were common. Our study, therefore, contributed to advancing gastric cancer molecular diagnostics and suggests clonal status is important to understanding gastric tumorigenesis. Our findings of a higher frequency of a poor prognosis associated molecular subtype in Latinos and a possible new aflatoxin gastric cancer etiology also advance cancer disparities research.
Significance: Our study contributes to advancing our knowledge of gastric carcinogenesis, diagnostics, and cancer health disparities.
© 2022 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
S. Urayama reports other from CellMax, Noah Medical, and Olympus America outside the submitted work. No disclosures were reported by the other authors.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Dagogo-Jack I, Shaw AT. Tumour heterogeneity and resistance to cancer therapies. Nat Rev Clin Oncol 2018;15:81–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
