

Clinical Pharmacology and Determinants of Response to UCART19, an Allogeneic Anti-CD19 CAR-T Cell Product, in Adult B-cell Acute Lymphoblastic Leukemia
- PMID: 36970059
- PMCID: PMC10035397
- DOI: 10.1158/2767-9764.CRC-22-0175
Clinical Pharmacology and Determinants of Response to UCART19, an Allogeneic Anti-CD19 CAR-T Cell Product, in Adult B-cell Acute Lymphoblastic Leukemia
Abstract
Background: UCART19 is an "off-the-shelf" genome-edited anti-CD19 chimeric antigen receptor (CAR)-T cell product, manufactured from unrelated healthy donor cells.
Methods: UCART19 was administered to 25 adult patients with relapsed or refractory (R/R) B-cell acute lymphoblastic leukemia (B-ALL) in the CALM trial. All patients underwent lymphodepletion with fludarabine and cyclophosphamide ± alemtuzumab and received one of three ascending doses of UCART19. Given the allogeneic nature of UCART19, we analyzed the impact of lymphodepletion, HLA disparities, and host immune system reconstitution on its kinetics, along with other factors known to affect autologous CAR-T cell clinical pharmacology.
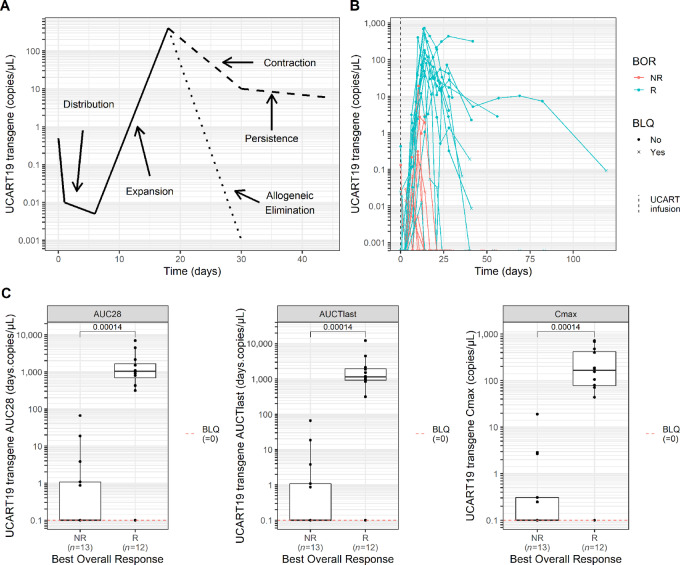
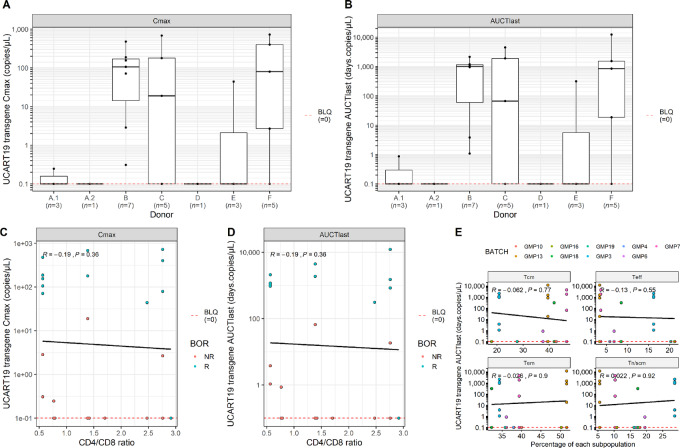
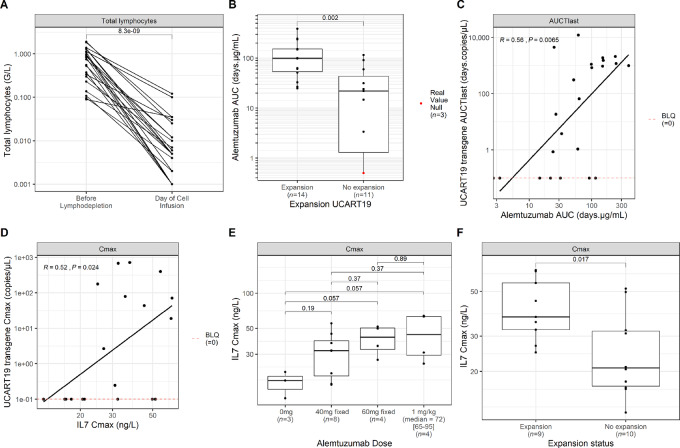
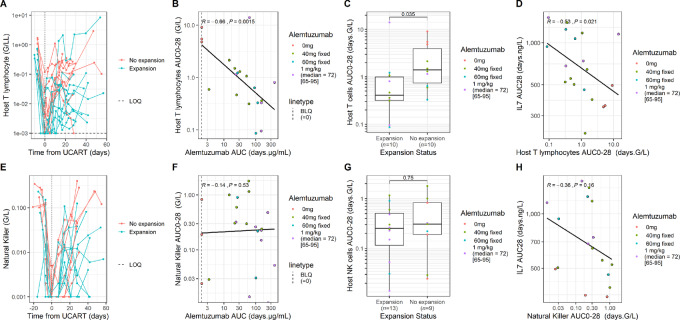
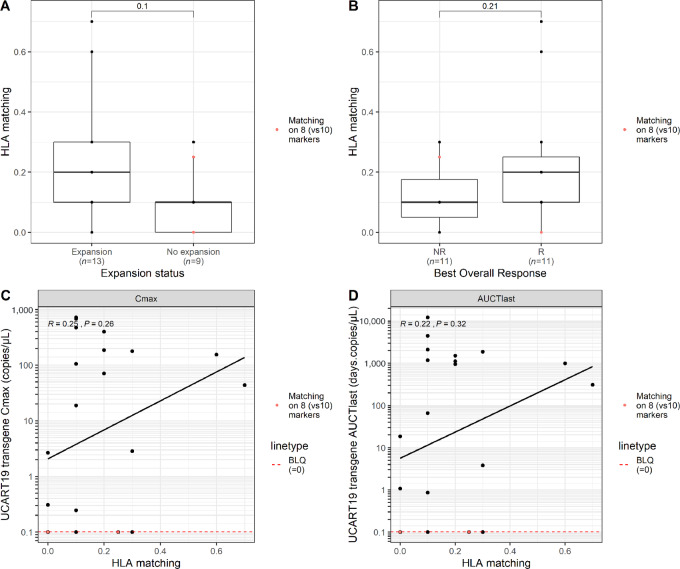
Results: Responder patients (12/25) had higher UCART19 expansion (C max) and exposure (AUCTlast) than nonresponders (13/25), as measured by transgene levels in peripheral blood. The persistence of CAR+ T cells did not exceed 28 days in 10/25 patients and lasted beyond 42 days in 4/25. No significant correlation was found between UCART19 kinetics and administered cell dose, patient and product characteristics or HLA disparities. However, the number of prior lines of therapy and absence of alemtuzumab negatively impacted UCART19 expansion and persistence. Alemtuzumab exposure positively affected IL7 and UCART19 kinetics, while negatively correlating with host T lymphocyte AUC0-28.
Conclusions: UCART19 expansion is a driver of response in adult patients with R/R B-ALL. These results shed light on the factors associated with UCART19 kinetics, which remain highly affected by the impact of alemtuzumab on IL7 and host-versus-graft rejection.
Significance: First description of the clinical pharmacology of a genome-edited allogeneic anti-CD19 CAR-T cell product showing the crucial role of an alemtuzumab-based regimen in sustaining UCART19 expansion and persistence through increased IL7 availability and decreased host T lymphocyte population.
© 2022 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
S. Dupouy reports personal fees from Servier and other from Allogene Therapeutics during the conduct of the study; personal fees from Servier outside the submitted work. I. Marchiq reports other from Allogene Therapeutics during the conduct of the study; and I. Marchiq is an employee of Servier. T. Derippe reports grants from Servier during the conduct of the study; grants from Servier outside the submitted work. M. Almena-Carrasco reports personal fees from Servier Laboratoires and other from Allogene Therapeutics during the conduct of the study; personal fees from Servier Laboratoires outside the submitted work. S. Fouliard reports personal fees from Servier and other from Allogene Therapeutics during the conduct of the study; personal fees from Servier outside the submitted work. J. Geronimi reports personal fees from Servier and other from Allogene Therapeutics during the conduct of the study; personal fees from Servier outside the submitted work. C. Graham reports grants from Servier during the conduct of the study. N. Jain reports grants, personal fees, and non-financial support from Servier during the conduct of the study; grants, personal fees, and non-financial support from Cellectis, Precision Biosciences, Abbvie, Genentech, Loxo Oncology, Fate Therapeutics; grants from Takeda outside the submitted work. M.V. Maus reports other from 2Seventy Bio outside the submitted work; in addition, M.V. Maus has a patent to Patents in CAR T cells for multiple indications pending; and M.V. Maus is an inventor on patents related to adoptive cell therapies, held by Massachusetts General Hospital (some licensed to Promab) and University of Pennsylvania (some licensed to Novartis). M.V. Maus holds Equity in 2SeventyBio, Century Therapeutics, Neximmune, Oncternal, and TCR2 and has served as a consultant for multiple companies involved in cell therapies; board of directors: 2Seventy Bio; M.V. Maus is a consultant for: Adaptimmune, Agenus, Allogene, Arcellx, Astellas, AstraZeneca, Atara, Bayer, BMS, Cabaletta Bio (SAB), Cellectis (SAB), CRISPR therapeutics, Genocea, In8bio (SAB), Intellia, GSK, Kite Pharma, Micromedicine/BendBio, Neximmune, Novartis, Oncternal, Sanofi, TCR2 (SAB), Tmunity, and WindMIL (SAB); M.V. Maus has had Grant/Research support : CRISPR therapeutics, Kite Pharma, Servier, Novartis; speaker's bureau: none. M. Mohty reports grants and personal fees from Jazz, Janssen, Sanofi; personal fees from Amgen, Takeda, Pfizer, Adaptive, Novartis, Astellas, GSK, Oncopeptides, and BMS outside the submitted work. N. Boissel reports personal fees from SERVIER during the conduct of the study; grants and personal fees from AMGEN; personal fees from Pfizer, Gilead, and Novartis outside the submitted work. T. Teshima reports grants from Sanofi, Chugai, Astellas, Teijin Pharma, Fuji Pharma, Nippon Shinyaku; personal fees from Merck Sharp & Dohme, Pfizer, Bristol-Myers Squibb; grants and personal fees from Kyowa Kirin; non-financial support from Janssen; grants, personal fees, and non-financial support from Novartis, and personal fees from Takeda outside the submitted work. K. Kato reports grants from Kyowa-Kirin, Novartis, Chugai, Takeda, AbbVie, Eisai, Janssen, Bristol-Myers Squibb, Ono, and Daiichi Sankyo during the conduct of the study. R. Benjamin reports grants from Servier and Allogene during the conduct of the study. No disclosures were reported by the other authors.
Figures
References
-
- Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J, et al. . Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet 2020;396:839–52. - PubMed
-
- Moreno-Cortes E, Forero-Forero JV, Lengerke-Diaz PA, Castro JE. Chimeric antigen receptor T cell therapy in oncology - pipeline at a glance: analysis of the ClinicalTrials.gov database. Crit Rev Oncol Hematol 2021;159:103239. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
