

Intrapulmonary and Intracardiac Shunts in Adult COVID-19 Versus Non-COVID Acute Respiratory Distress Syndrome ICU Patients Using Echocardiography and Contrast Bubble Studies (COVID-Shunt Study): A Prospective, Observational Cohort Study
- PMID: 36971440
- PMCID: PMC10335602
- DOI: 10.1097/CCM.0000000000005848
Intrapulmonary and Intracardiac Shunts in Adult COVID-19 Versus Non-COVID Acute Respiratory Distress Syndrome ICU Patients Using Echocardiography and Contrast Bubble Studies (COVID-Shunt Study): A Prospective, Observational Cohort Study
Abstract
Objectives: Studies have suggested intrapulmonary shunts may contribute to hypoxemia in COVID-19 acute respiratory distress syndrome (ARDS) with worse associated outcomes. We evaluated the presence of right-to-left (R-L) shunts in COVID-19 and non-COVID ARDS patients using a comprehensive hypoxemia workup for shunt etiology and associations with mortality.
Design: Prospective, observational cohort study.
Setting: Four tertiary hospitals in Edmonton, Alberta, Canada.
Patients: Adult critically ill, mechanically ventilated, ICU patients admitted with COVID-19 or non-COVID (November 16, 2020, to September 1, 2021).
Interventions: Agitated-saline bubble studies with transthoracic echocardiography/transcranial Doppler ± transesophageal echocardiography assessed for R-L shunts presence.
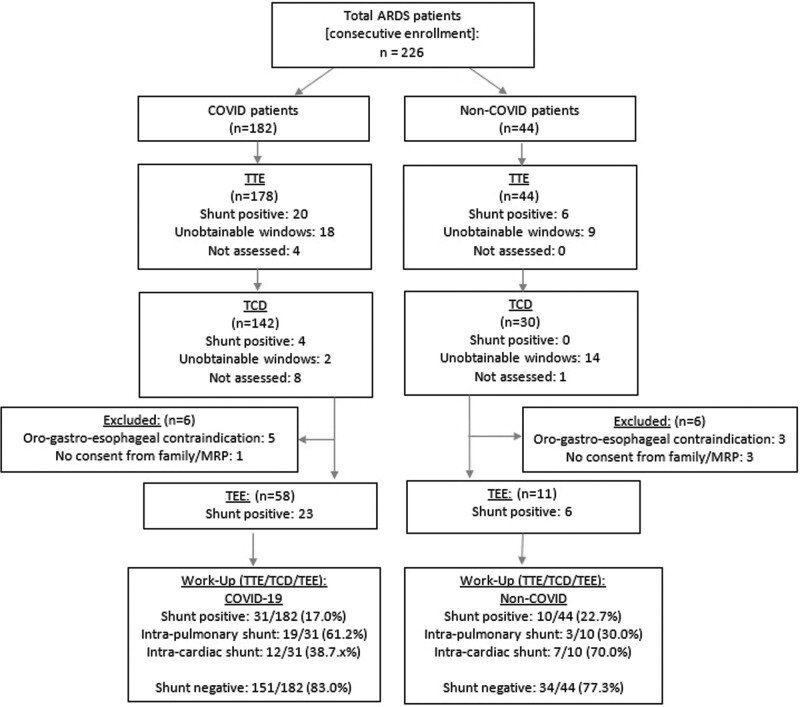
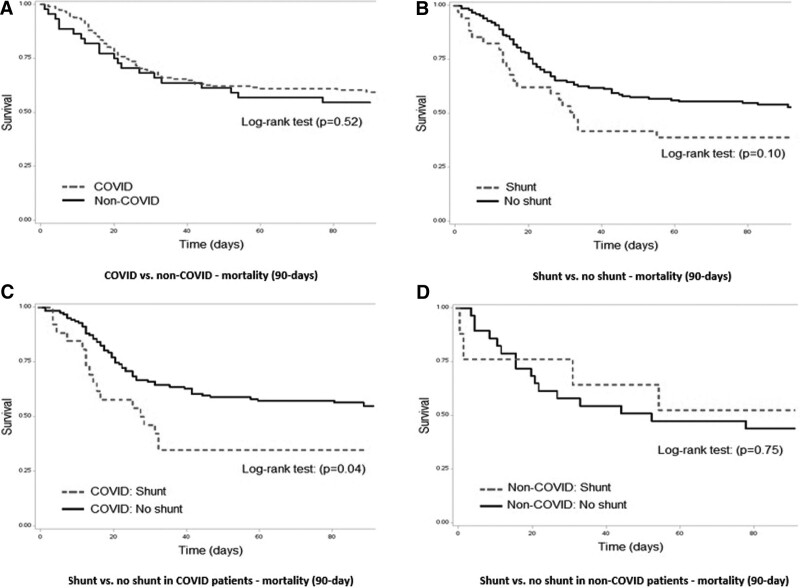
Measurements and main results: Primary outcomes were shunt frequency and association with hospital mortality. Logistic regression analysis was used for adjustment. The study enrolled 226 patients (182 COVID-19 vs 42 non-COVID). Median age was 58 years (interquartile range [IQR], 47-67 yr) and Acute Physiology and Chronic Health Evaluation II scores of 30 (IQR, 21-36). In COVID-19 patients, the frequency of R-L shunt was 31 of 182 COVID patients (17.0%) versus 10 of 44 non-COVID patients (22.7%), with no difference detected in shunt rates (risk difference [RD], -5.7%; 95% CI, -18.4 to 7.0; p = 0.38). In the COVID-19 group, hospital mortality was higher for those with R-L shunt compared with those without (54.8% vs 35.8%; RD, 19.0%; 95% CI, 0.1-37.9; p = 0.05). This did not persist at 90-day mortality nor after adjustment with regression.
Conclusions: There was no evidence of increased R-L shunt rates in COVID-19 compared with non-COVID controls. R-L shunt was associated with increased in-hospital mortality for COVID-19 patients, but this did not persist at 90-day mortality or after adjusting using logistic regression.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Lau’s institution received funding from the University Hospital Foundation, the Royal Alexandra Hospital Foundation, and the Covenant Health Foundation. Dr. Shaw received funding from Edwards Lifesciences, Novartis, and Astellas. Dr. Opgenorth disclosed that she is an employee of the University of Alberta. Dr. Bagshaw received funding from Baxter and BioPorto; he is supported by a Canada Research Chair in Critical Care Outcomes and Systems Evaluation. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Johns Hopkins Coronavirus Resource Center: COVID-19 Map. Available at: https://coronavirus.jhu.edu/map.html. Accessed July 27, 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
