Value Placed on Comfort vs Life Prolongation Among Patients Treated With Maintenance Dialysis
- PMID: 36972031
- PMCID: PMC10043804
- DOI: 10.1001/jamainternmed.2023.0265
Value Placed on Comfort vs Life Prolongation Among Patients Treated With Maintenance Dialysis
Abstract
Importance: Patients receiving maintenance dialysis experience intensive patterns of end-of-life care that might not be consistent with their values.
Objective: To evaluate the association of patients' health care values with engagement in advance care planning and end-of-life care.
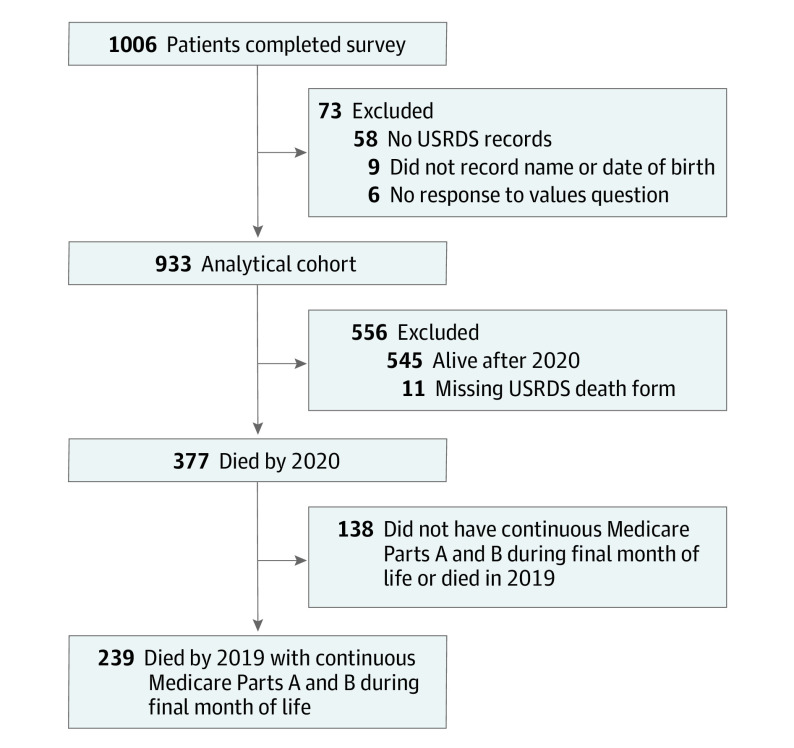
Design, setting, and participants: Survey study of patients who received maintenance dialysis between 2015 and 2018 at dialysis centers in the greater metropolitan areas of Seattle, Washington, and Nashville, Tennessee, with longitudinal follow-up of decedents. Logistic regression models were used to estimate probabilities. Data analysis was conducted between May and October 2022.
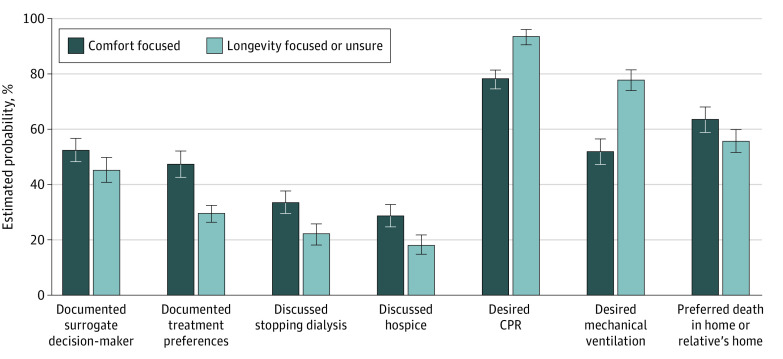
Exposures: A survey question about the value that the participant would place on longevity-focused vs comfort-focused care if they were to become seriously ill.
Main outcomes and measures: Self-reported engagement in advance care planning and care received near the end of life through 2020 using linked kidney registry data and Medicare claims.
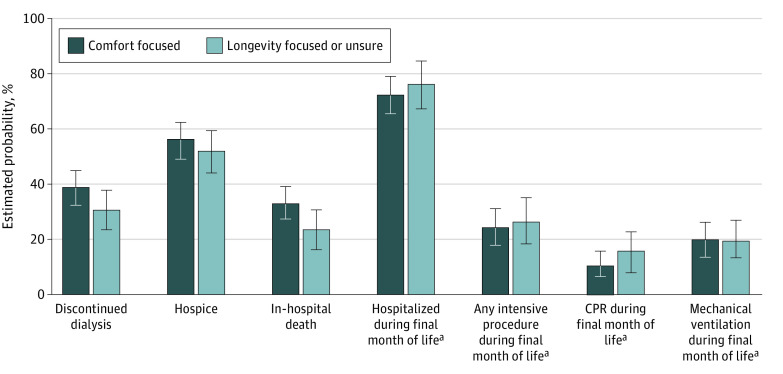
Results: Of 933 patients (mean [SD] age, 62.6 [14.0] years; 525 male patients [56.3%]; 254 [27.2%] identified as Black) who responded to the question about values and could be linked to registry data (65.2% response rate [933 of 1431 eligible patients]), 452 (48.4%) indicated that they would value comfort-focused care, 179 (19.2%) that they would value longevity-focused care, and 302 (32.4%) that they were unsure about the intensity of care they would value. Many had not completed an advance directive (estimated probability, 47.5% [95% CI, 42.9%-52.1%] of those who would value comfort-focused care vs 28.1% [95% CI, 24.0%-32.3%] of those who would value longevity-focused care or were unsure; P < .001), had not discussed hospice (estimated probability, 28.6% [95% CI, 24.6%-32.9%] comfort focused vs 18.2% [95% CI, 14.7%-21.7%] longevity focused or unsure; P < .001), or had not discussed stopping dialysis (estimated probability, 33.3% [95% CI, 29.0%-37.7%] comfort focused vs 21.9% [95% CI, 18.2%-25.8%] longevity focused or unsure; P < .001). Most respondents wanted to receive cardiopulmonary resuscitation (estimated probability, 78.0% [95% CI, 74.2%-81.7%] comfort focused vs 93.9% [95% CI, 91.4%-96.1%] longevity focused or unsure; P < .001) and mechanical ventilation (estimated probability, 52.0% [95% CI, 47.4%-56.6%] comfort focused vs 77.9% [95% CI, 74.0%-81.7%] longevity focused or unsure; P < .001). Among decedents, the percentages of participants who received an intensive procedure during the final month of life (estimated probability, 23.5% [95% CI, 16.5%-31.0%] comfort focused vs 26.1% [95% CI, 18.0%-34.5%] longevity focused or unsure; P = .64), discontinued dialysis (estimated probability, 38.3% [95% CI, 32.0%-44.8%] comfort focused vs 30.2% [95% CI, 23.0%-37.8%] longevity focused or unsure; P = .09), and enrolled in hospice (estimated probability, 32.2% [95% CI, 25.7%-38.7%] comfort focused vs 23.3% [95% CI, 16.4%-30.5%] longevity focused or unsure; P = .07) were not statistically different.
Conclusions and relevance: This survey study found that there appeared to be a disconnect between patients' expressed values, which were largely comfort focused, and their engagement in advance care planning and end-of-life care, which reflected a focus on longevity. These findings suggest important opportunities to improve the quality of care for patients receiving dialysis.
Conflict of interest statement
Figures