

Comparative Effectiveness of Fludrocortisone and Hydrocortisone vs Hydrocortisone Alone Among Patients With Septic Shock
- PMID: 36972033
- PMCID: PMC10043800
- DOI: 10.1001/jamainternmed.2023.0258
Comparative Effectiveness of Fludrocortisone and Hydrocortisone vs Hydrocortisone Alone Among Patients With Septic Shock
Abstract
Importance: Patients with septic shock may benefit from the initiation of corticosteroids. However, the comparative effectiveness of the 2 most studied corticosteroid regimens (hydrocortisone with fludrocortisone vs hydrocortisone alone) is unclear.
Objective: To compare the effectiveness of adding fludrocortisone to hydrocortisone vs hydrocortisone alone among patients with septic shock using target trial emulation.
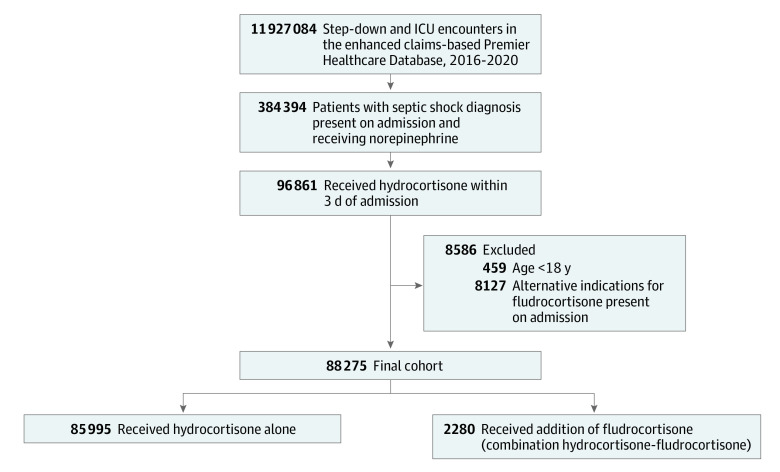
Design, setting, and participants: This retrospective cohort study from 2016 to 2020 used the enhanced claims-based Premier Healthcare Database, which included approximately 25% of US hospitalizations. Participants were adult patients hospitalized with septic shock and receiving norepinephrine who began hydrocortisone treatment. Data analysis was performed from May 2022 to December 2022.
Exposure: Addition of fludrocortisone on the same calendar day that hydrocortisone treatment was initiated vs use of hydrocortisone alone.
Main outcome and measures: Composite of hospital death or discharge to hospice. Adjusted risk differences were calculated using doubly robust targeted maximum likelihood estimation.
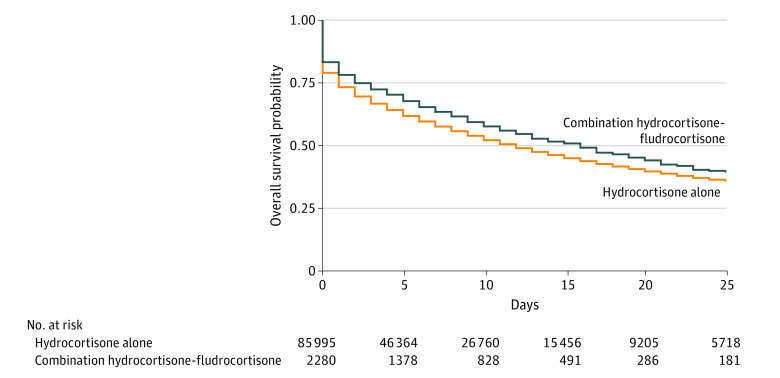
Results: Analyses included 88 275 patients, 2280 who began treatment with hydrocortisone-fludrocortisone (median [IQR] age, 64 [54-73] years; 1041 female; 1239 male) and 85 995 (median [IQR] age, 67 [57-76] years; 42 136 female; 43 859 male) who began treatment with hydrocortisone alone. The primary composite outcome of death in hospital or discharge to hospice occurred among 1076 (47.2%) patients treated with hydrocortisone-fludrocortisone vs 43 669 (50.8%) treated with hydrocortisone alone (adjusted absolute risk difference, -3.7%; 95% CI, -4.2% to -3.1%; P < .001).
Conclusions and relevance: In this comparative effectiveness cohort study among adult patients with septic shock who began hydrocortisone treatment, the addition of fludrocortisone was superior to hydrocortisone alone.
Conflict of interest statement
Figures
Comment in
-
Should We Add Fludrocortisone to Hydrocortisone for Treatment of Septic Shock?JAMA Intern Med. 2023 May 1;183(5):460-461. doi: 10.1001/jamainternmed.2023.0257. JAMA Intern Med. 2023. PMID: 36972044 No abstract available.
