

Timing of Allergenic Food Introduction and Risk of Immunoglobulin E-Mediated Food Allergy: A Systematic Review and Meta-analysis
- PMID: 36972063
- PMCID: PMC10043805
- DOI: 10.1001/jamapediatrics.2023.0142
Timing of Allergenic Food Introduction and Risk of Immunoglobulin E-Mediated Food Allergy: A Systematic Review and Meta-analysis
Abstract
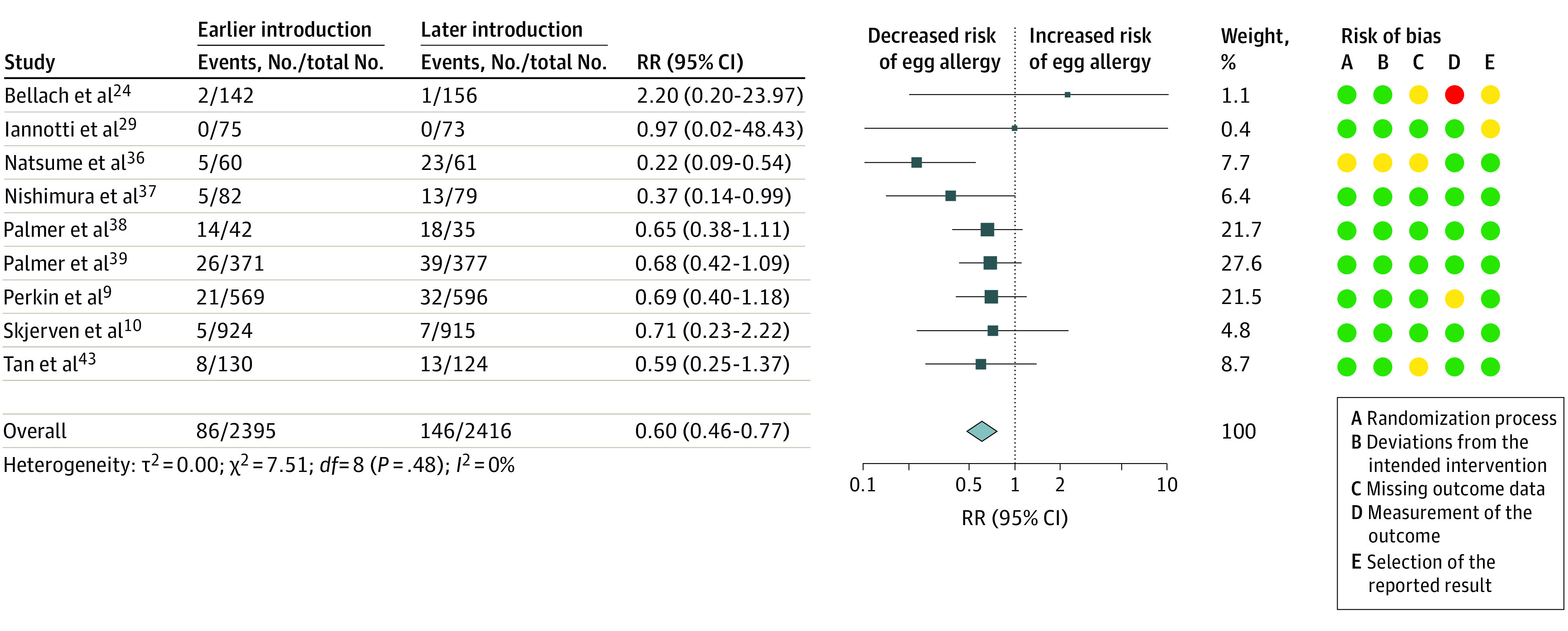
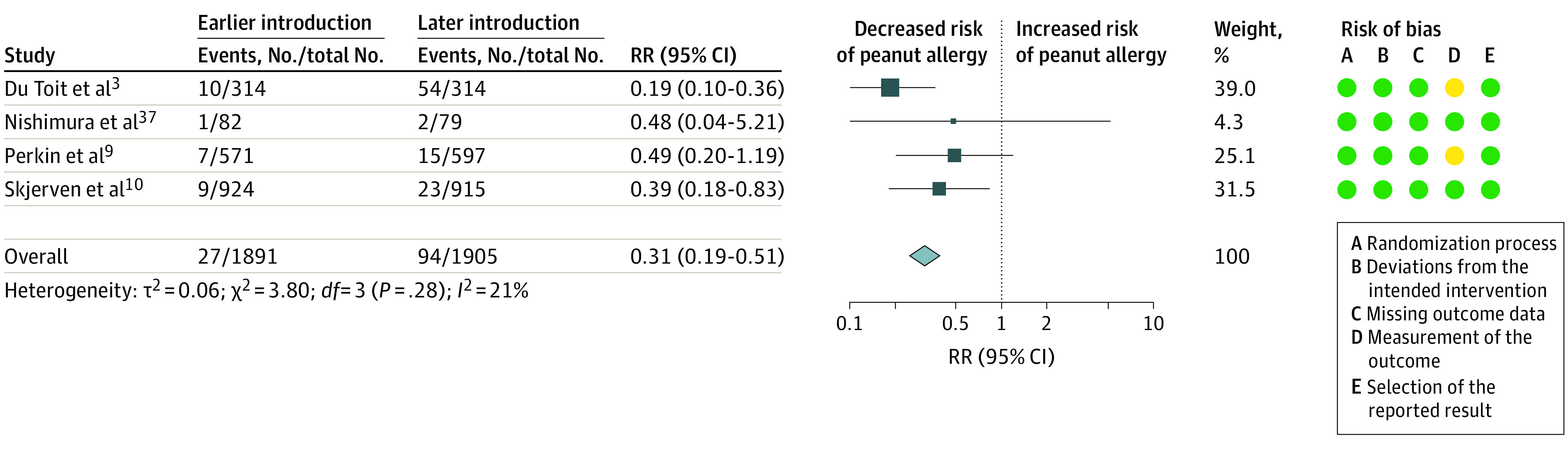
Importance: Earlier egg and peanut introduction probably reduces risk of egg and peanut allergy, respectively, but it is uncertain whether food allergy as a whole can be prevented using earlier allergenic food introduction.
Objective: To investigate associations between timing of allergenic food introduction to the infant diet and risk of food allergy.
Data sources: In this systematic review and meta-analysis, Medline, Embase, and CENTRAL databases were searched for articles from database inception to December 29, 2022. Search terms included infant, randomized controlled trial, and terms for common allergenic foods and allergic outcomes.
Study selection: Randomized clinical trials evaluating age at allergenic food introduction (milk, egg, fish, shellfish, tree nuts, wheat, peanuts, and soya) during infancy and immunoglobulin E (IgE)-mediated food allergy from 1 to 5 years of age were included. Screening was conducted independently by multiple authors.
Data extraction and synthesis: The Preferred Reporting Items for Systematic Reviews and Meta-analyses guideline was used. Data were extracted in duplicate and synthesized using a random-effects model. The Grading of Recommendations, Assessment, Development, and Evaluation framework was used to assess certainty of evidence.
Main outcomes and measures: Primary outcomes were risk of IgE-mediated allergy to any food from 1 to 5 years of age and withdrawal from the intervention. Secondary outcomes included allergy to specific foods.
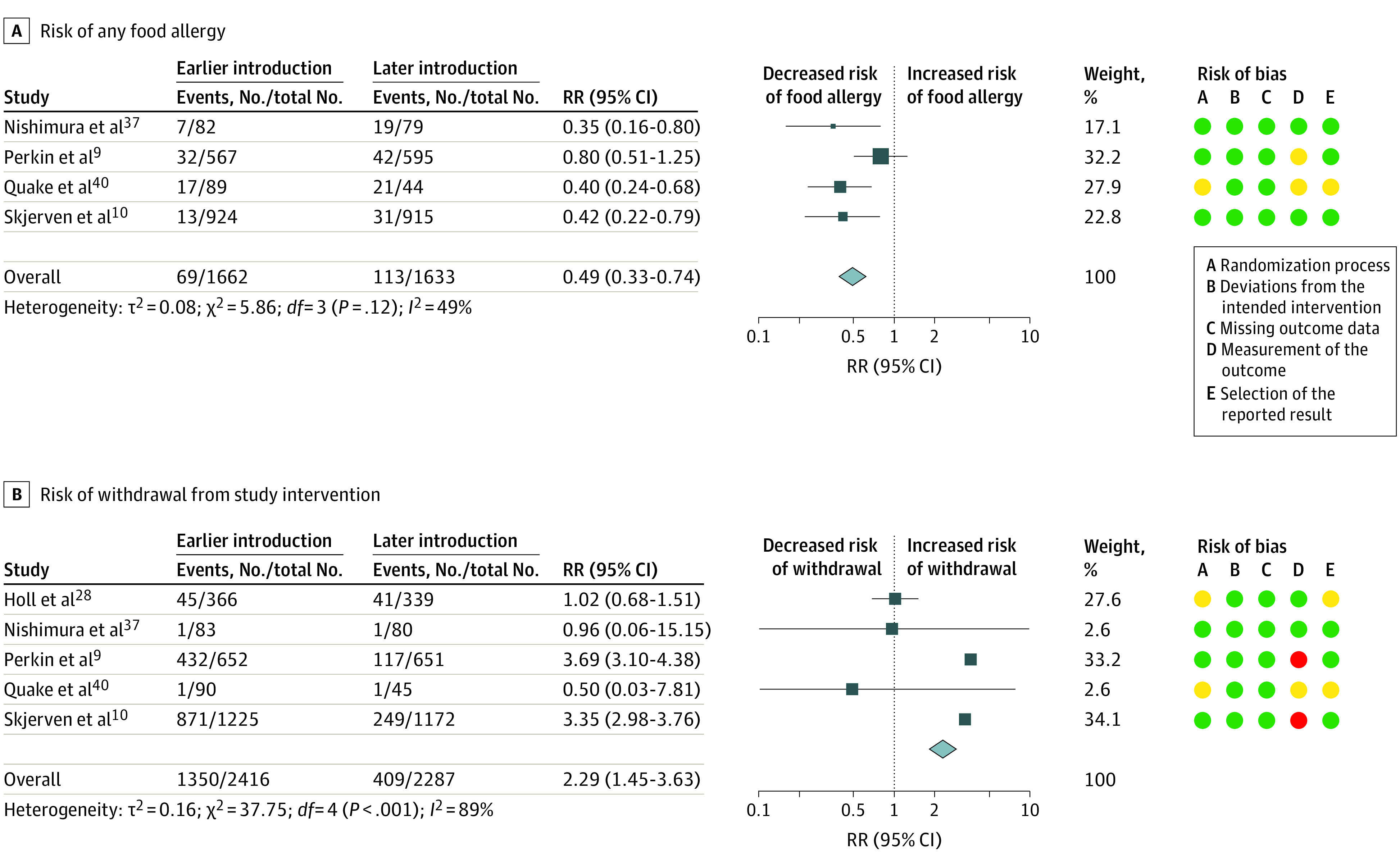
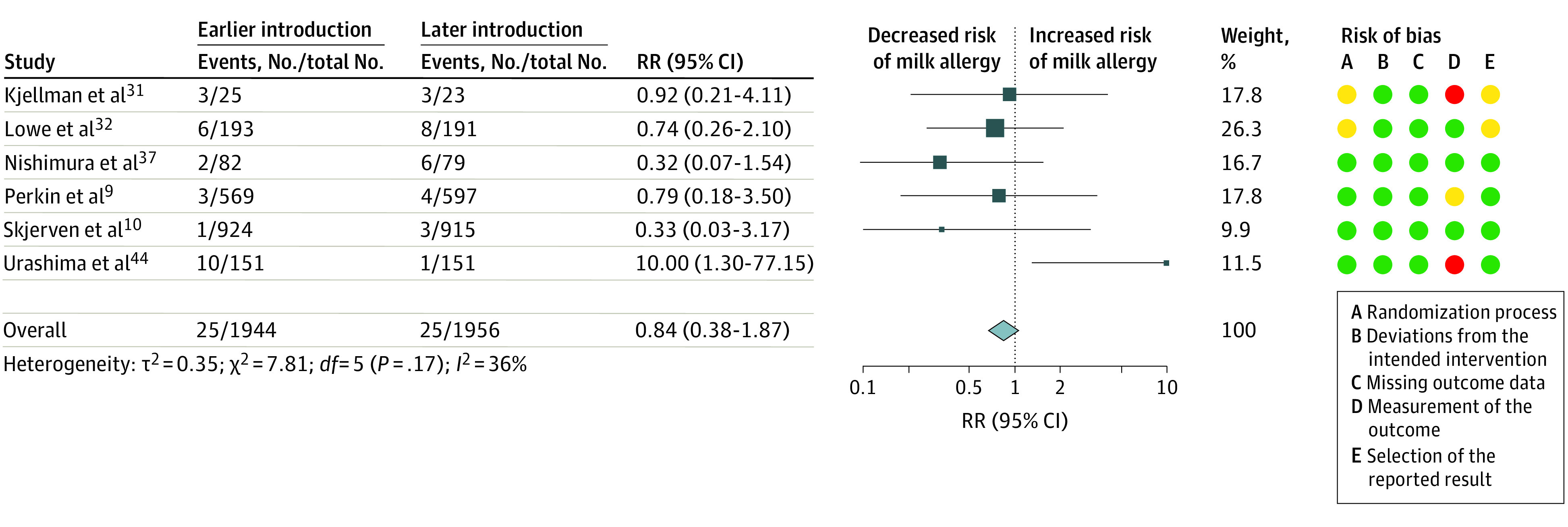
Results: Of 9283 titles screened, data were extracted from 23 eligible trials (56 articles, 13 794 randomized participants). There was moderate-certainty evidence from 4 trials (3295 participants) that introduction of multiple allergenic foods from 2 to 12 months of age (median age, 3-4 months) was associated with reduced risk of food allergy (risk ratio [RR], 0.49; 95% CI, 0.33-0.74; I2 = 49%). Absolute risk difference for a population with 5% incidence of food allergy was -26 cases (95% CI, -34 to -13 cases) per 1000 population. There was moderate-certainty evidence from 5 trials (4703 participants) that introduction of multiple allergenic foods from 2 to 12 months of age was associated with increased withdrawal from the intervention (RR, 2.29; 95% CI, 1.45-3.63; I2 = 89%). Absolute risk difference for a population with 20% withdrawal from the intervention was 258 cases (95% CI, 90-526 cases) per 1000 population. There was high-certainty evidence from 9 trials (4811 participants) that introduction of egg from 3 to 6 months of age was associated with reduced risk of egg allergy (RR, 0.60; 95% CI, 0.46-0.77; I2 = 0%) and high-certainty evidence from 4 trials (3796 participants) that introduction of peanut from 3 to 10 months of age was associated with reduced risk of peanut allergy (RR, 0.31; 95% CI, 0.19-0.51; I2 = 21%). Evidence for timing of introduction of cow's milk and risk of cow's milk allergy was very low certainty.
Conclusions and relevance: In this systematic review and meta-analysis, earlier introduction of multiple allergenic foods in the first year of life was associated with lower risk of developing food allergy but a high rate of withdrawal from the intervention. Further work is needed to develop allergenic food interventions that are safe and acceptable for infants and their families.
Conflict of interest statement
Figures
Comment in
-
Data Extraction and Handling Issues on Evidence Synthesis of Risk of Immunoglobulin E-Mediated Food Allergy.JAMA Pediatr. 2023 Sep 1;177(9):983. doi: 10.1001/jamapediatrics.2023.2465. JAMA Pediatr. 2023. PMID: 37486627 No abstract available.
-
Data Extraction and Handling Issues on Evidence Synthesis of Risk of Immunoglobulin E-Mediated Food Allergy-Reply.JAMA Pediatr. 2023 Sep 1;177(9):984. doi: 10.1001/jamapediatrics.2023.2462. JAMA Pediatr. 2023. PMID: 37486639 No abstract available.
References
-
- Du Toit G, Sayre PH, Roberts G, et al. ; Immune Tolerance Network Learning Early About Peanut Allergy study team . Allergen specificity of early peanut consumption and effect on development of allergic disease in the Learning Early About Peanut Allergy study cohort. J Allergy Clin Immunol. 2018;141(4):1343-1353. doi:10.1016/j.jaci.2017.09.034 - DOI - PMC - PubMed
-
- Halken S, Muraro A, de Silva D, et al. ; European Academy of Allergy and Clinical Immunology Food Allergy and Anaphylaxis Guidelines Group . EAACI guideline: preventing the development of food allergy in infants and young children (2020 update). Pediatr Allergy Immunol. 2021;32(5):843-858. doi:10.1111/pai.13496 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
