

Diagnosis and treatment for gastro-oesophageal cancer in England and Wales: analysis of the National Oesophago-Gastric Cancer Audit (NOGCA) database 2012-2020
- PMID: 36972221
- PMCID: PMC10364547
- DOI: 10.1093/bjs/znad065
Diagnosis and treatment for gastro-oesophageal cancer in England and Wales: analysis of the National Oesophago-Gastric Cancer Audit (NOGCA) database 2012-2020
Abstract
Background: The National Oesophago-Gastric Cancer Audit (NOGCA) captures patient data from diagnosis to end of primary treatment for all patients with oesophagogastric (OG) cancer in England and Wales. This study assessed changes in patient characteristics, treatments received, and outcomes for OG cancer surgery for the period 2012-2020, and examined which factors may have led to changes in clinical outcomes over this time.
Methods: Patients diagnosed with OG cancer between April 2012 and March 2020 were included. Descriptive statistics were used to summarize patient demographics, disease site, type, and stage, patterns of care, and outcomes over time. The treatment variables of unit case volume, surgical approach, and neoadjuvant therapy were included. Regression models were used to examine associations between surgical outcomes (duration of stay and mortality), and patient and treatment variables.
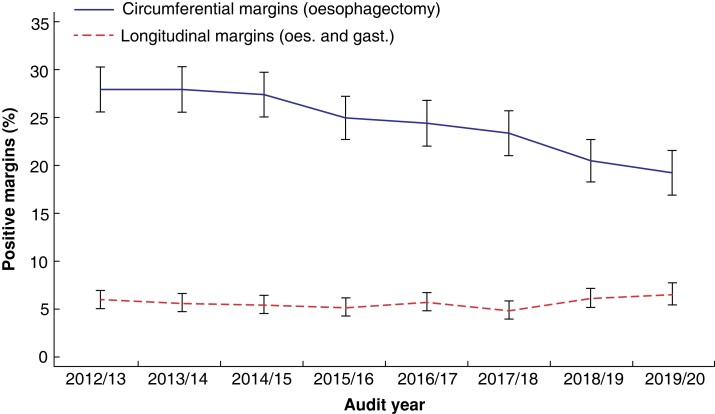
Results: In total, 83 393 patients diagnosed with OG cancer during the study period were included. Patient demographics and cancer stage at diagnosis showed little change over time. Altogether, 17 650 patients underwent surgery as part of radical treatment. These patients had increasingly more advanced cancers, and a greater likelihood of pre-existing comorbidity in more recent years. Significant decreases in mortality rates and duration of stay were noted, along with improvements in oncological outcomes (nodal yields and margin positivity rates). Following adjustment for patient and treatment variables, increasing audit year and trust volume were associated, respectively, with improved postoperative outcomes: lower 30-day mortality (odds ratio (OR) 0.93 (95 per cent c.i. 0.88 to 0.98) and OR 0.99 (95 per cent c.i. 0.99-0.99)) and lower 90-day mortality (OR 0.94 (95 per cent c.i. 0.91 to 0.98) and OR 0.99 (95 per cent c.i. 0.99-0.99)), and a reduction in duration of postoperative stay (incidence rate ratio (IRR) 0.98 (95 per cent c.i. 0.97 to 0.98) and IRR 0.99 (95 per cent c.i. 0.99 to 0.99)).
Conclusion: Outcomes of OG cancer surgery have improved over time, despite little evidence of improvements in early diagnosis. The underlying drivers for improvements in outcome are multifactorial.
© The Author(s) 2023. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures

References
-
- van der Sluis PC, van der Horst S, May AM, Schippers C, Brosens LAA, Joore HCAet al. . Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer: a randomized controlled trial. Ann Surg 2019;269:621–630 - PubMed
-
- Biere SSAY, Van Berge Henegouwen MI, Maas KW, Bonavina L, Rosman C, Garcia JRet al. . Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet 2012;379:1887–1892 - PubMed
-
- Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper Set al. . Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet 2019;393:1948–1957 - PubMed
-
- Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPLet al. . Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol 2015;16:1090–1098 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
