

Magnetothermal-based non-invasive focused magnetic stimulation for functional recovery in chronic stroke treatment
- PMID: 36973390
- PMCID: PMC10042827
- DOI: 10.1038/s41598-023-31979-w
Magnetothermal-based non-invasive focused magnetic stimulation for functional recovery in chronic stroke treatment
Abstract
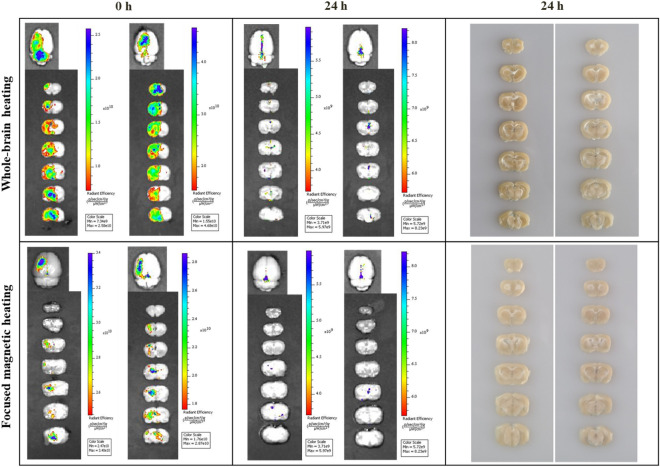
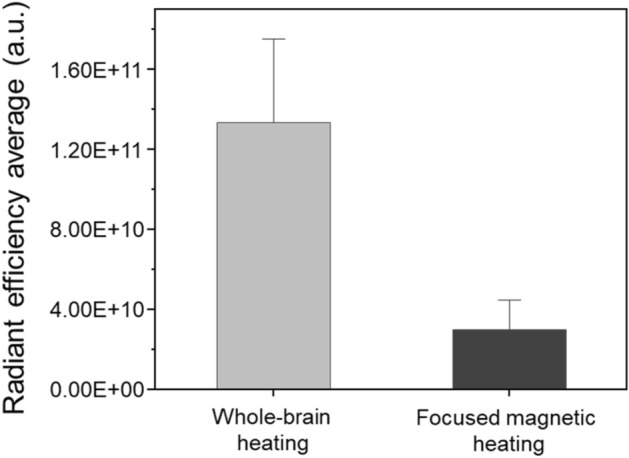
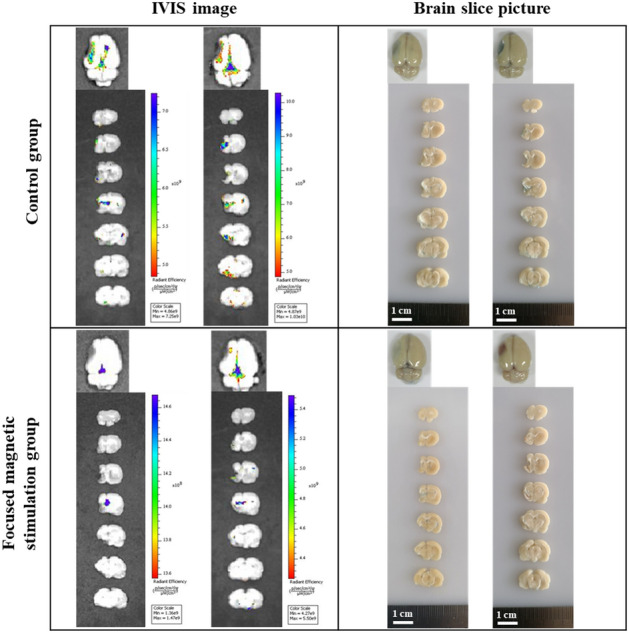
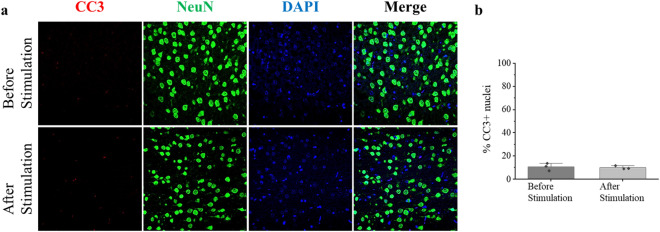
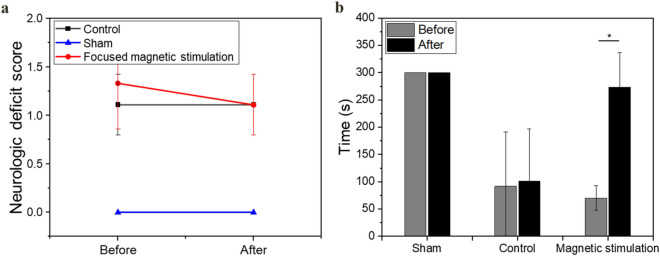
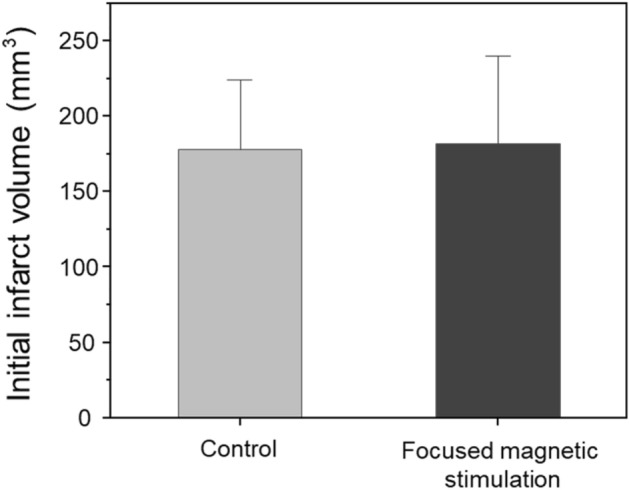
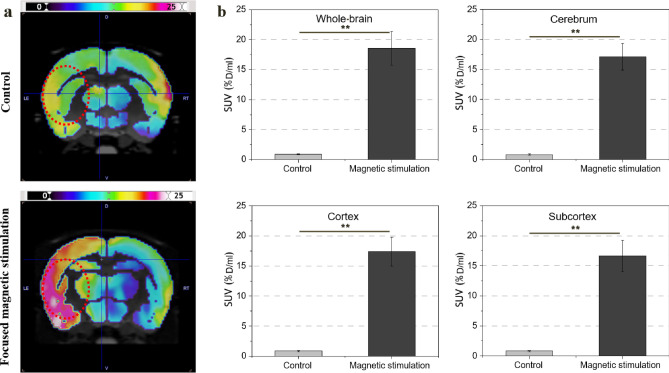
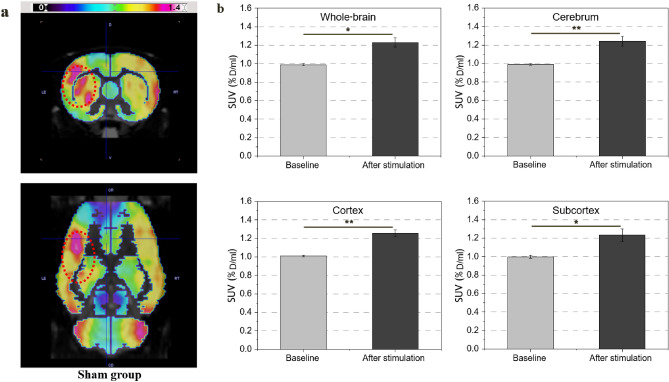
Magnetic heat-based brain stimulation of specific lesions could promote the restoration of impaired motor function caused by chronic stroke. We delivered localized stimulation by nanoparticle-mediated heat generation within the targeted brain area via focused magnetic stimulation. The middle cerebral artery occlusion model was prepared, and functional recovery in the chronic-phase stroke rat model was demonstrated by the therapeutic application of focused magnetic stimulation. We observed a transient increase in blood-brain barrier permeability at the target site of < 4 mm and metabolic brain activation at the target lesion. After focused magnetic stimulation, the rotarod score increased by 390 ± 28% (p < 0.05) compared to the control group. Standardized uptake value in the focused magnetic stimulation group increased by 2063 ± 748% (p < 0.01) compared to the control group. Moreover, an increase by 24 ± 5% (p < 0.05) was observed in the sham group as well. Our results show that non-invasive focused magnetic stimulation can safely modulate BBB permeability and enhance neural activation for chronic-phase stroke treatment in the targeted deep brain area.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
