

Effectiveness of artificial intelligence screening in preventing vision loss from diabetes: a policy model
- PMID: 36973403
- PMCID: PMC10042864
- DOI: 10.1038/s41746-023-00785-z
Effectiveness of artificial intelligence screening in preventing vision loss from diabetes: a policy model
Abstract
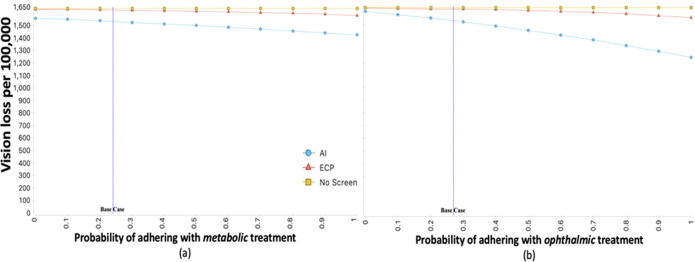
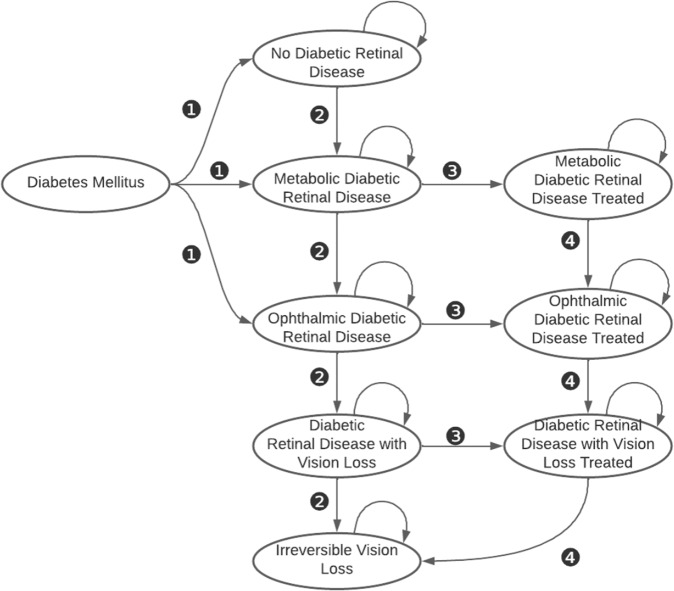
The effectiveness of using artificial intelligence (AI) systems to perform diabetic retinal exams ('screening') on preventing vision loss is not known. We designed the Care Process for Preventing Vision Loss from Diabetes (CAREVL), as a Markov model to compare the effectiveness of point-of-care autonomous AI-based screening with in-office clinical exam by an eye care provider (ECP), on preventing vision loss among patients with diabetes. The estimated incidence of vision loss at 5 years was 1535 per 100,000 in the AI-screened group compared to 1625 per 100,000 in the ECP group, leading to a modelled risk difference of 90 per 100,000. The base-case CAREVL model estimated that an autonomous AI-based screening strategy would result in 27,000 fewer Americans with vision loss at 5 years compared with ECP. Vision loss at 5 years remained lower in the AI-screened group compared to the ECP group, in a wide range of parameters including optimistic estimates biased toward ECP. Real-world modifiable factors associated with processes of care could further increase its effectiveness. Of these factors, increased adherence with treatment was estimated to have the greatest impact.
© 2023. The Author(s).
Conflict of interest statement
R.C.: none. R.W.: Research support Dexcom. M.D.A.: reports the following competing interests: Investor, Director, Consultant of Digital Diagnostics Inc, Coralville, IA; patents and patent applications assigned to the University of Iowa and Digital Diagnostics that are relevant to the subject matter of this paper. H.P.L.: None.
Figures

References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
