

Study protocol for a randomized controlled trial of Proportional Assist Ventilation for Minimizing the Duration of Mechanical Ventilation: the PROMIZING study
- PMID: 36973743
- PMCID: PMC10041480
- DOI: 10.1186/s13063-023-07163-w
Study protocol for a randomized controlled trial of Proportional Assist Ventilation for Minimizing the Duration of Mechanical Ventilation: the PROMIZING study
Abstract
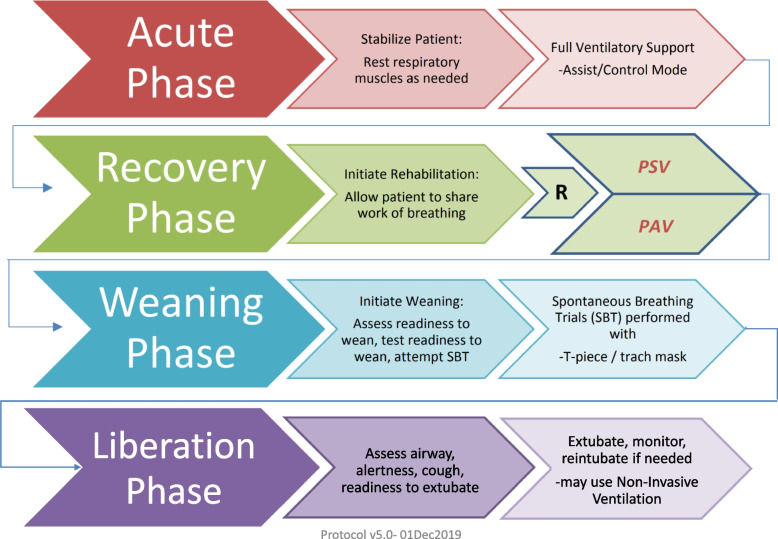
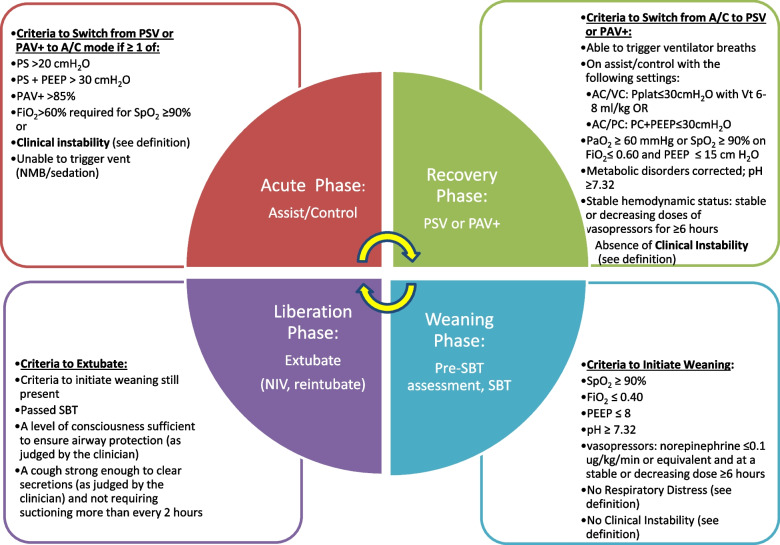
Background: Proportional assist ventilation with load-adjustable gain factors (PAV+) is a mechanical ventilation mode that delivers assistance to breathe in proportion to the patient's effort. The proportional assistance, called the gain, can be adjusted by the clinician to maintain the patient's respiratory effort or workload within a normal range. Short-term and physiological benefits of this mode compared to pressure support ventilation (PSV) include better patient-ventilator synchrony and a more physiological response to changes in ventilatory demand.
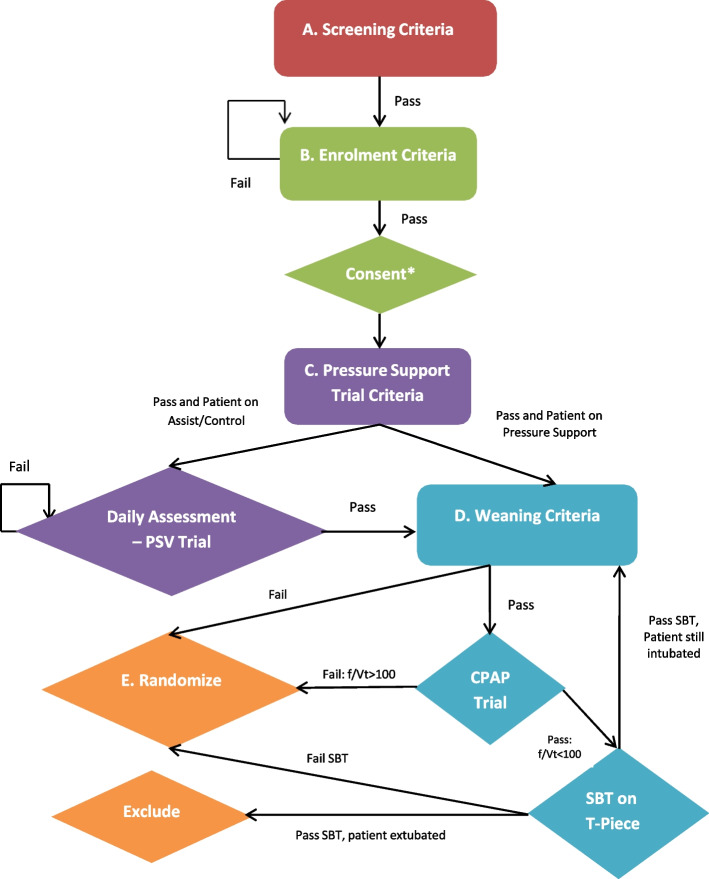
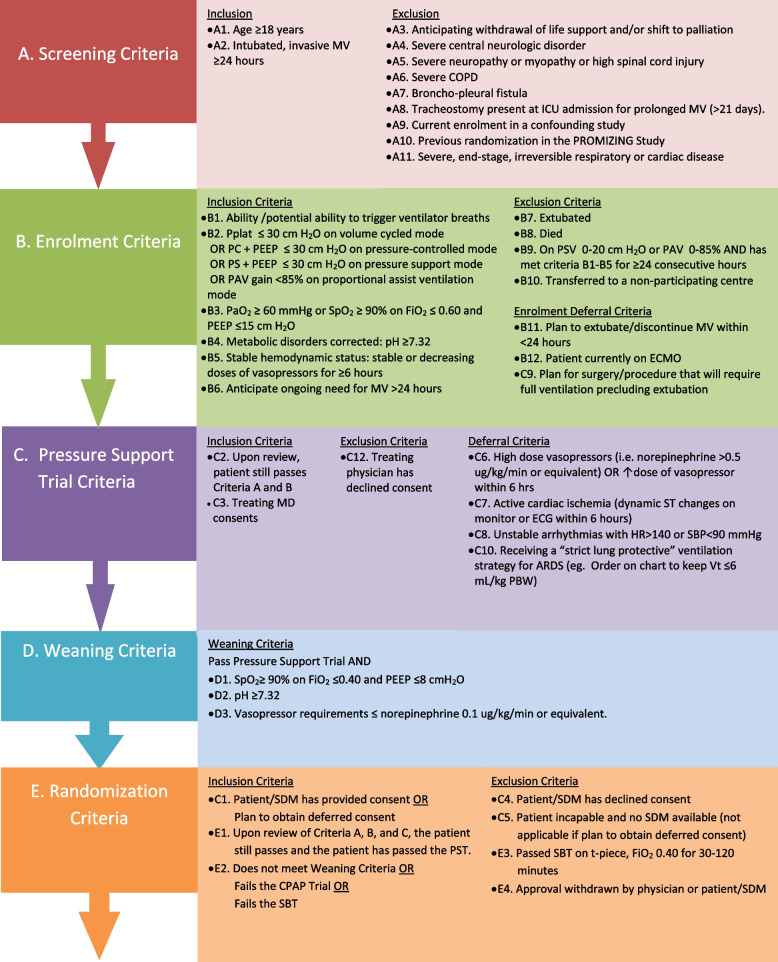
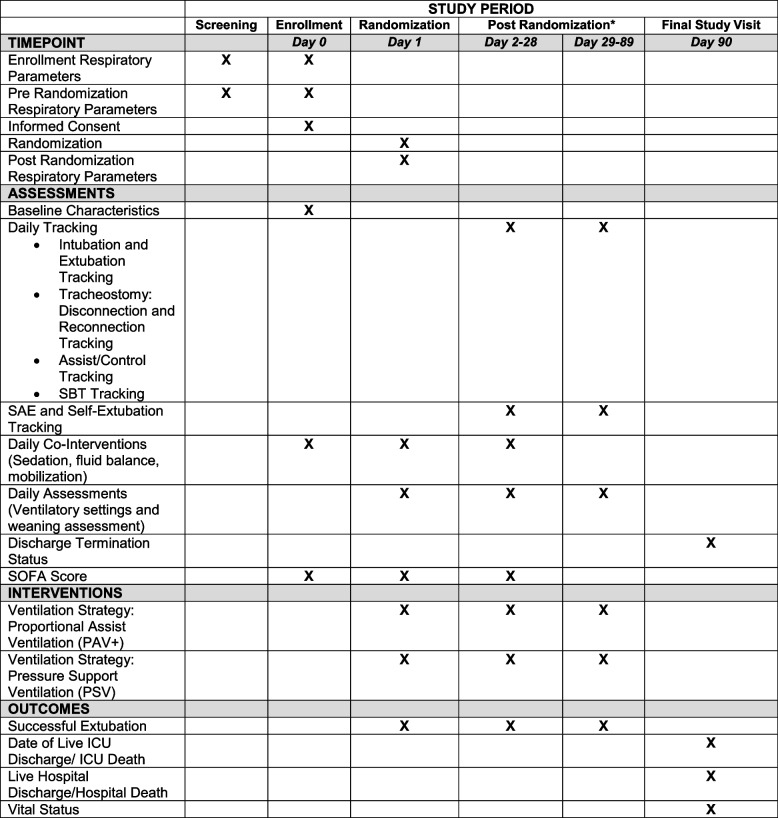
Methods: The objective of this multi-centre randomized controlled trial (RCT) is to determine if, for patients with acute respiratory failure, ventilation with PAV+ will result in a shorter time to successful extubation than with PSV. This multi-centre open-label clinical trial plans to involve approximately 20 sites in several continents. Once eligibility is determined, patients must tolerate a short-term PSV trial and either (1) not meet general weaning criteria or (2) fail a 2-min Zero Continuous Positive Airway Pressure (CPAP) Trial using the rapid shallow breathing index, or (3) fail a spontaneous breathing trial (SBT), in this sequence. Then, participants in this study will be randomized to either PSV or PAV+ in a 1:1 ratio. PAV+ will be set according to a target of muscular pressure. The weaning process will be identical in the two arms. Time to liberation will be the primary outcome; ventilator-free days and other outcomes will be measured.
Discussion: Meta-analyses comparing PAV+ to PSV suggest PAV+ may benefit patients and decrease healthcare costs but no powered study to date has targeted the difficult to wean patient population most likely to benefit from the intervention, or used consistent timing for the implementation of PAV+. Our enrolment strategy, primary outcome measure, and liberation approaches may be useful for studying mechanical ventilation and weaning and can offer important results for patients.
Trial registration: ClinicalTrials.gov NCT02447692 . Prospectively registered on May 19, 2015.
Keywords: Patient-ventilatory synchrony; Proportional assist ventilation; Ventilator-free days; Weaning from mechanical ventilation; Work of breathing.
© 2023. The Author(s).
Conflict of interest statement
The authors declare they have no direct competing interests in the study. The study received partial industry funding through the first grant which was a CIHR-industry partnership, with the industry partner at arm’s length. The industry partner, Medtronic, has no role in the study design, data collection, analysis, interpretation or publication of manuscript. No author received personal financial remuneration for the study. The authors declare no other competing interests in the study.
Figures
References
-
- Jaber S, Petrof BJ, Jung B, Chanques G, Berthet JP, Rabuel C, et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am J Respir Crit Care Med. 2011;183(3):364–71. - PubMed
-
- Levine S, Nguyen T, Taylor N, Friscia ME, Budak MT, Rothenberg P, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008;358(13):1327–35. - PubMed
-
- Bosma K, Ferreyra G, Ambrogio C, Pasero D, Mirabella L, Braghiroli A, et al. Patient-ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med. 2007;35(4):1048–54. - PubMed
-
- Thille AW, Rodriguez P, Cabello B, Lellouche F, Brochard L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006;32(10):1515–22. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
