

Neuroendocrine carcinoma of the minor papilla with pancreas divisum: a case report and review of the literature
- PMID: 36973791
- PMCID: PMC10044798
- DOI: 10.1186/s13256-023-03828-x
Neuroendocrine carcinoma of the minor papilla with pancreas divisum: a case report and review of the literature
Abstract
Background: Neuroendocrine tumors of the minor papilla are very rare, and only 20 cases have been reported in the literature. Neuroendocrine carcinoma of the minor papilla with pancreas divisum has not been reported previously, making this the first reported case. Neuroendocrine tumors of the minor papilla have been reported in association with pancreas divisum in about 50% of cases reported in the literature. We herein present our case of neuroendocrine carcinoma of the minor papilla with pancreas divisum in a 75-year-old male with a systematic literature review of the previous 20 reports of neuroendocrine tumors of the minor papilla.
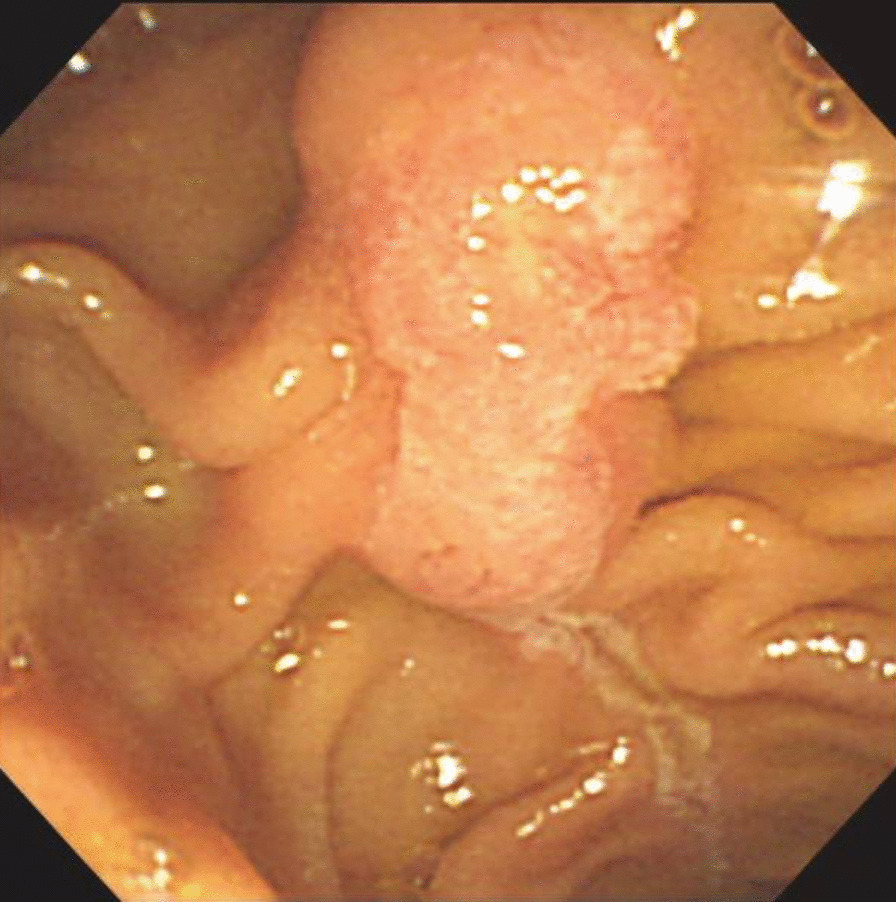
Case presentation: A 75-year-old Asian man was referred to our hospital for evaluation of dilation of the main pancreatic duct noted on abdominal ultrasonography. Magnetic resonance cholangiopancreatography and endoscopic retrograde cholangiopancreatography showed a dilated dorsal pancreatic duct, which was not connected to the ventral pancreatic duct; however, it opened to the minor papilla, indicating pancreas divisum. The common bile duct had no communication with the pancreatic main duct and opened to the ampulla of Vater. A contrast-enhanced computed tomography scan showed a 12-mm hypervascular mass near the ampulla of Vater. Endoscopic ultrasonography showed a defined hypoechoic mass in the minor papilla with no invasion. The biopsies performed at the previous hospital found adenocarcinoma. The patient underwent a subtotal stomach-preserving pancreaticoduodenectomy. The pathological diagnosis was neuroendocrine carcinoma. At the 15-year follow-up visit, the patient was doing well with no evidence of tumor recurrence.
Conclusion: In our case, because the tumor was discovered during a medical check-up relatively early in the course of disease, the patient was doing well at the 15-year follow-up visit, with no evidence of tumor recurrence. Diagnosing a tumor of the minor papilla is very difficult because of the relatively small size and submucosal location. Carcinoids and endocrine cell micronests in the minor papilla occur more frequently than generally thought. It is very important to include neuroendocrine tumors of the minor papilla in the differential diagnosis of patients with recurrent pancreatitis or pancreatitis of unknown cause, especially for patients with pancreas divisum.
Keywords: Minor papilla; Neuroendocrine carcinoma; Neuroendocrine tumor; Pancreas divisum; Pancreatitis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
A case of pancreas divisum with marked dilatation of dorsal pancreatic duct.Clin J Gastroenterol. 2022 Dec;15(6):1204-1209. doi: 10.1007/s12328-022-01713-6. Epub 2022 Oct 5. Clin J Gastroenterol. 2022. PMID: 36197567 Review.
-
Carcinoid tumor of the minor papilla in complete pancreas divisum presenting as recurrent abdominal pain.BMC Gastroenterol. 2010 Feb 12;10:17. doi: 10.1186/1471-230X-10-17. BMC Gastroenterol. 2010. PMID: 20149263 Free PMC article.
-
Intraductal papillary mucinous carcinoma of the pancreas associated with pancreas divisum: a case report and review of the literature.BMC Gastroenterol. 2015 Jul 8;15:78. doi: 10.1186/s12876-015-0313-3. BMC Gastroenterol. 2015. PMID: 26152300 Free PMC article. Review.
-
Adenocarcinoma of the minor duodenal papilla with intraepithelial spread to the pancreatic duct.Virchows Arch. 2007 Dec;451(6):1075-81. doi: 10.1007/s00428-007-0496-2. Epub 2007 Sep 6. Virchows Arch. 2007. PMID: 17805567
-
[Endoscopic therapy of pancreas divisum].Orv Hetil. 1998 Nov 15;139(46):2761-4. Orv Hetil. 1998. PMID: 9849061 Hungarian.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
