

Non-eosinophilic asthma in nonsteroidal anti-inflammatory drug exacerbated respiratory disease
- PMID: 36973957
- PMCID: PMC10009799
- DOI: 10.1002/clt2.12235
Non-eosinophilic asthma in nonsteroidal anti-inflammatory drug exacerbated respiratory disease
Abstract
Background: The cellular inflammatory pattern of nonsteroidal anti-inflammatory drug-exacerbated respiratory disease (N-ERD) is heterogeneous. However, data on the heterogeneity of non-eosinophilic asthma (NEA) with aspirin hypersensitivity are scanty. By examination of N-ERD patients based on clinical data and eicosanoid biomarkers we aimed to identify NEA endotypes potentially guiding clinical management.
Methods: Induced sputum was collected from patients with N-ERD. Sixty six patients (49.6% of 133 N-ERD) with NEA were included in the hierarchical cluster analysis based on clinical and laboratory data. The quality of clustering was evaluated using internal cluster validation with different indices and a practical decision tree was proposed to simplify stratification of patients.
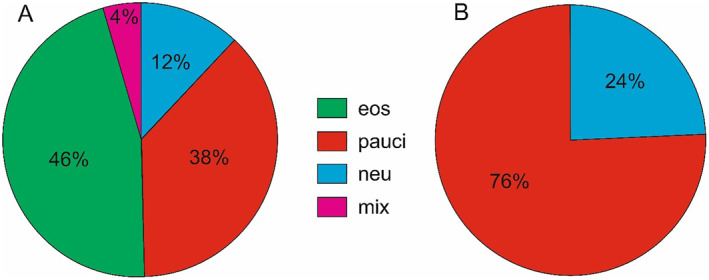
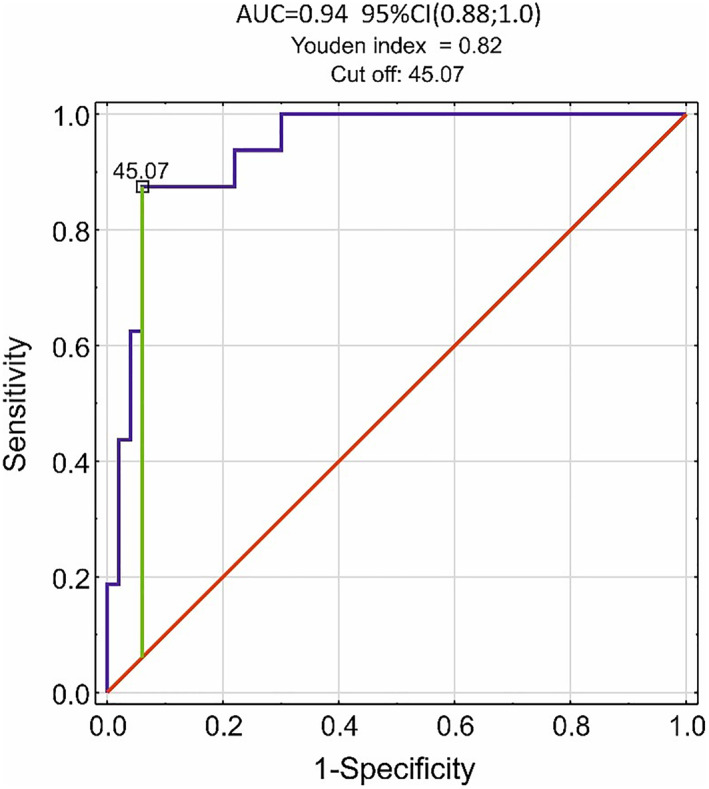
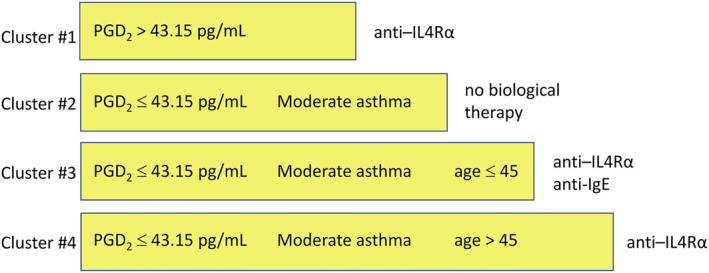
Results: The most frequent NEA pattern was paucigranulocytic (PGA; 75.8%), remaining was neutrophilic asthma (NA; 24.2%). Four clusters were identified. Cluster #3 included the highest number of NEA patients (37.9%) with severe asthma and PGA pattern (96.0%). Cluster #1 (24.2%) included severe only asthma, with a higher prevalence of NA (50%). Cluster #2 (25.8%) comprised well-controlled mild or severe asthma (PGA; 76.5%). Cluster #4 contained only 12.1% patients with well-controlled moderate asthma (PGA; 62.5%). Sputum prostaglandin D2 levels distinguished cluster #1 from the remaining clusters with an area under the curve of 0.94.
Conclusions: Among identified four NEA subtypes, clusters #3 and #1 represented N-ERD patients with severe asthma but a different inflammatory signatures. All the clusters were discriminated by sputum PGD2 levels, asthma severity, and age of patients. The heterogeneity of non-eosinophilic N-ERD suggests a need for novel targeted interventions.
Keywords: aspirin hypersensitivity; cluster analysis; inflammatory phenotypes; non-eosinophilic asthma.
© 2023 The Authors. Clinical and Translational Allergy published by John Wiley & Sons Ltd on behalf of European Academy of Allergy and Clinical Immunology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Heterogeneity of Paucigranulocytic Asthma: A Prospective Cohort Study with Hierarchical Cluster Analysis.J Allergy Clin Immunol Pract. 2021 Jun;9(6):2344-2355. doi: 10.1016/j.jaip.2021.01.004. Epub 2021 Jan 20. J Allergy Clin Immunol Pract. 2021. PMID: 33482419
-
Heterogeneity of lower airway inflammation in patients with NSAID-exacerbated respiratory disease.J Allergy Clin Immunol. 2021 Apr;147(4):1269-1280. doi: 10.1016/j.jaci.2020.08.007. Epub 2020 Aug 15. J Allergy Clin Immunol. 2021. PMID: 32810516
-
Endotypes of severe neutrophilic and eosinophilic asthma from multi-omics integration of U-BIOPRED sputum samples.Clin Transl Med. 2024 Jul;14(7):e1771. doi: 10.1002/ctm2.1771. Clin Transl Med. 2024. PMID: 39073027 Free PMC article.
-
Monoclonal antibody or aspirin desensitization in NSAID-exacerbated respiratory disease (N-ERD)?Front Allergy. 2023 Apr 12;4:1080951. doi: 10.3389/falgy.2023.1080951. eCollection 2023. Front Allergy. 2023. PMID: 37123562 Free PMC article. Review.
-
Paucigranulocytic asthma: Uncoupling of airway obstruction from inflammation.J Allergy Clin Immunol. 2019 Apr;143(4):1287-1294. doi: 10.1016/j.jaci.2018.06.008. Epub 2018 Jun 19. J Allergy Clin Immunol. 2019. PMID: 29928921 Free PMC article. Review.
Cited by
-
Clinical and mechanistic advancements in aspirin exacerbated respiratory disease.J Allergy Clin Immunol. 2025 May;155(5):1411-1419. doi: 10.1016/j.jaci.2025.03.006. Epub 2025 Mar 18. J Allergy Clin Immunol. 2025. PMID: 40113018 Review.
-
Low Prostaglandin E2 but High Prostaglandin D2, a Paradoxical Dissociation in Arachidonic Acid Metabolism in Aspirin-Exacerbated Airway Disease: Role of Airway Epithelium.J Clin Med. 2024 Dec 5;13(23):7416. doi: 10.3390/jcm13237416. J Clin Med. 2024. PMID: 39685875 Free PMC article. Review.
-
Unique effect of aspirin on local 15-oxo-eicosatetraenoic acid synthesis in asthma patients with aspirin hypersensitivity.Clin Transl Allergy. 2024 Dec;14(12):e70004. doi: 10.1002/clt2.70004. Clin Transl Allergy. 2024. PMID: 39722441 Free PMC article.
-
Aspirin hypersensitivity diagnostic index (AHDI): In vitro test for diagnosing of N-ERD based on urinary 15-oxo-ETE and LTE4 excretion.Allergy. 2025 Feb;80(2):534-544. doi: 10.1111/all.16281. Epub 2024 Aug 23. Allergy. 2025. PMID: 39180224 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
