

A clinician-to-clinician universal electronic consultation programme at the cardiology department of a Galician healthcare area improves healthcare accessibility and outcomes in elderly patients
- PMID: 36974264
- PMCID: PMC10039426
- DOI: 10.1093/ehjdh/ztad004
A clinician-to-clinician universal electronic consultation programme at the cardiology department of a Galician healthcare area improves healthcare accessibility and outcomes in elderly patients
Abstract
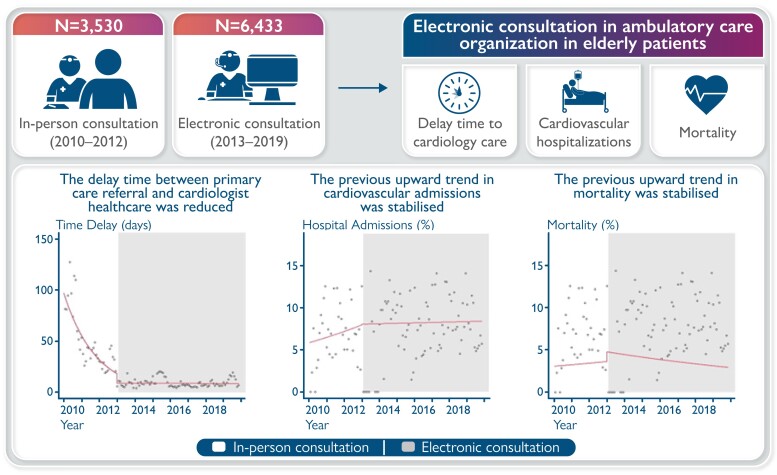
Aims: We aimed to assess longer-term results (accessibility, hospital admissions, and mortality) in elderly patients referred to a cardiology department (CD) from primary care using e-consultation in outpatient care.
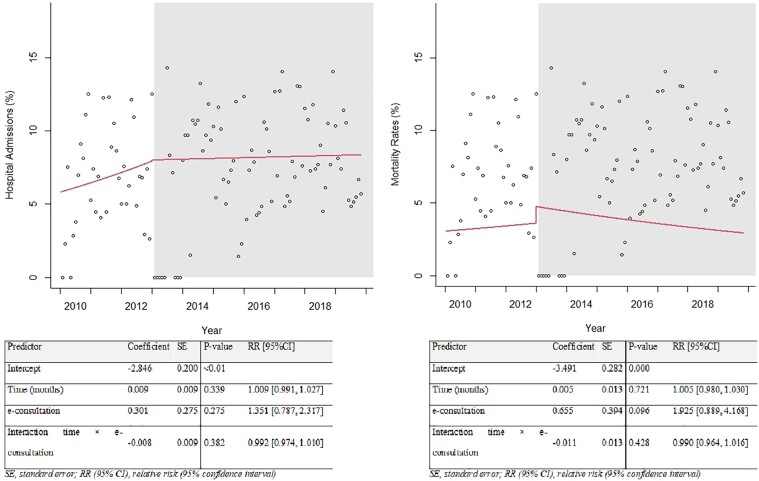
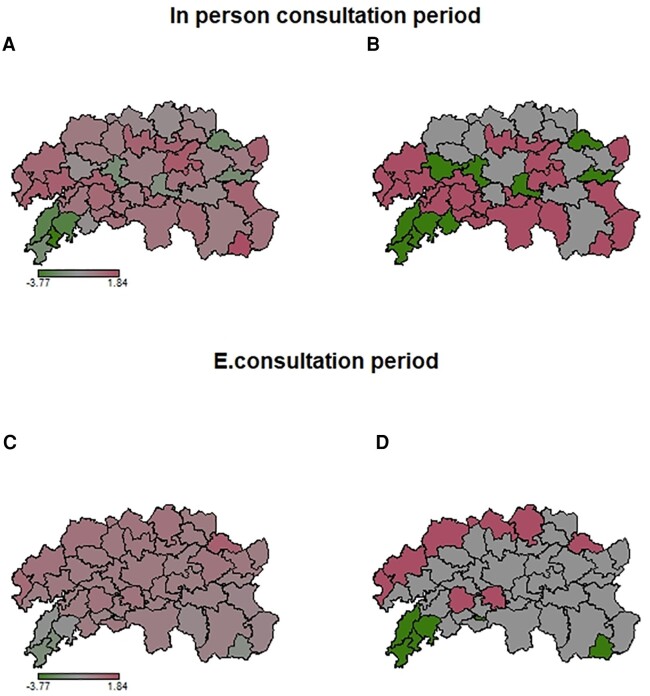
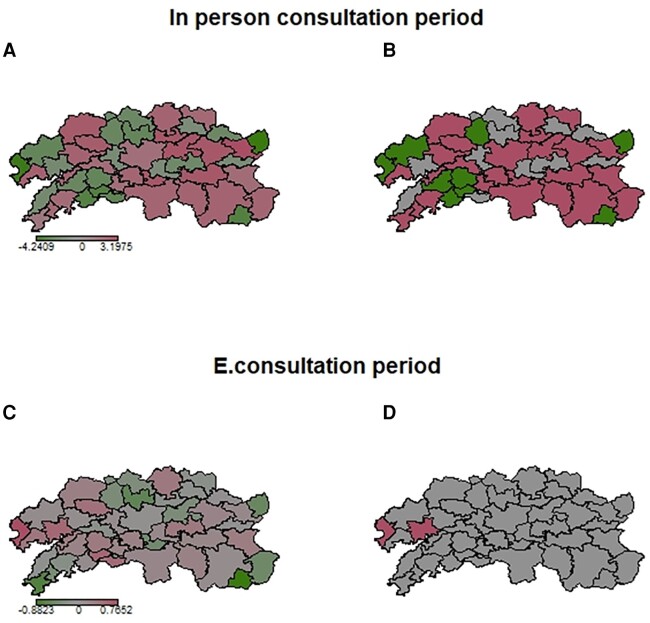
Methods and results: We included 9963 patients >80 years from 1 January 2010 to 31 December 2019. Until 2012, all patients attended an in-person consultation (2010-2012). In 2013, we instituted an e-consult programme (2013-2019) for all primary care referrals to cardiologists that preceded a patient's in-person consultation when considered. We used an interrupted time series (ITS) regression approach to investigate the impact of e-consultation on (i) cardiovascular hospital admissions and mortality. We also analysed (ii) the total number and referral rate (population-adjusted referred rate) in both periods, and (iii) the accessibility was measured as the number of consultations and variation according to the distance from the municipality and reference hospital. During e-consultation, the demand for care increased (12.8 ± 4.3% vs. 25.5 ± 11.1% per 1000 inhabitants, P < 0.001) and referrals from different areas were equalized. After the implementation of e-consultation, we observed that the increase in hospital admissions and mortality were stabilized [incidence rate ratio (iRR): 1.351 (95% CI, 0.787, 2.317), P = 0.874] and [iRR: 1.925 (95% CI: 0.889, 4.168), P = 0.096], respectively. The geographic variabilities in hospital admissions and mortality seen during the in-person consultation were stabilized after e-consultation implementation.
Conclusions: Implementation of a clinician-to-clinician e-consultation programme in outpatient care was associated with improved accessibility to cardiology healthcare in elderly patients. After e-consultations were implemented, hospital admissions and mortality were stabilized.
Keywords: Elderly; Electronic consultation; Healthcare; Outcomes health.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: The authors declare no conflicts of interest in relation to this article.
Figures
Similar articles
-
Longer-Term Results of a Universal Electronic Consultation Program at the Cardiology Department of a Galician Healthcare Area.Circ Cardiovasc Qual Outcomes. 2022 Jan;15(1):e008130. doi: 10.1161/CIRCOUTCOMES.121.008130. Epub 2022 Jan 18. Circ Cardiovasc Qual Outcomes. 2022. PMID: 35041483
-
Gender differences on healthcare accessibility and outcomes of a electronic inter-clinician consultation program at the cardiology department in a Galician Health Area.Eur J Clin Invest. 2023 Sep;53(9):e14012. doi: 10.1111/eci.14012. Epub 2023 May 8. Eur J Clin Invest. 2023. PMID: 37114978
-
The impact of inter-clinician electronic consultation in patients diagnosed with atrial fibrillation in primary care.Eur J Clin Invest. 2023 Mar;53(3):e13904. doi: 10.1111/eci.13904. Epub 2022 Nov 24. Eur J Clin Invest. 2023. PMID: 36346678
-
Evaluating mental health decision units in acute care pathways (DECISION): a quasi-experimental, qualitative and health economic evaluation.Health Soc Care Deliv Res. 2023 Dec;11(25):1-221. doi: 10.3310/PBSM2274. Health Soc Care Deliv Res. 2023. PMID: 38149657
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.Health Technol Assess. 2004 Dec;8(50):1-106, iii-iv. doi: 10.3310/hta8500. Health Technol Assess. 2004. PMID: 15546515 Review.
Cited by
-
Impact of a clinician-to-clinician electronic consultation in heart failure patients with previous hospital admissions.Eur Heart J Digit Health. 2023 Nov 7;5(1):9-20. doi: 10.1093/ehjdh/ztad052. eCollection 2024 Jan. Eur Heart J Digit Health. 2023. PMID: 38264693 Free PMC article.
References
-
- Oseran AS, Wasfy JH. Early experiences with cardiology electronic consults: a systematic review. Am Heart J 2019;215:139–146. - PubMed
-
- Rey-Aldana D, Cinza-Sanjurjo S, Portela-Romero M, López-Barreiro JL, Garcia-Castelo A, Pazos-Mareque JM, et al. . Programa de consulta electrónica universal (e-consulta) de un servicio de cardiología. Resultados a largo plazo. Rev Esp Cardiol 2022;75:159–165. - PubMed
-
- Rey-Aldana D, Mazón-Ramos P, Portela-Romero M, Cinza-Sanjurjo S, Alvarez-Alvarez B, Agra-Bermejo R, et al. . Longer-Term results of a universal electronic consultation program at the cardiology department of a galician healthcare area. Circ Cardiovasc Qual Outcomes 2022;15:16–24. - PubMed
-
- Rey Aldana D, Reyes Santias F, Mazón Ramos P, Portela Romero M, Cinza Sanjurjo S, Álvarez Álvarez B, et al. . Cost and potential savings of electronic consultation and its relationship with reduction in atmospheric pollution. Sustainability 2021;13:12436.
LinkOut - more resources
Full Text Sources