

A Cost-Effectiveness Analysis of the Various Treatment Options for Distal Radius Fractures
- PMID: 36974282
- PMCID: PMC10039314
- DOI: 10.1016/j.jhsg.2022.11.007
A Cost-Effectiveness Analysis of the Various Treatment Options for Distal Radius Fractures
Abstract
Purpose: To conduct a cost-effectiveness study of nonsurgical and surgical treatment options for distal radius fractures using distinct posttreatment outcome patterns.
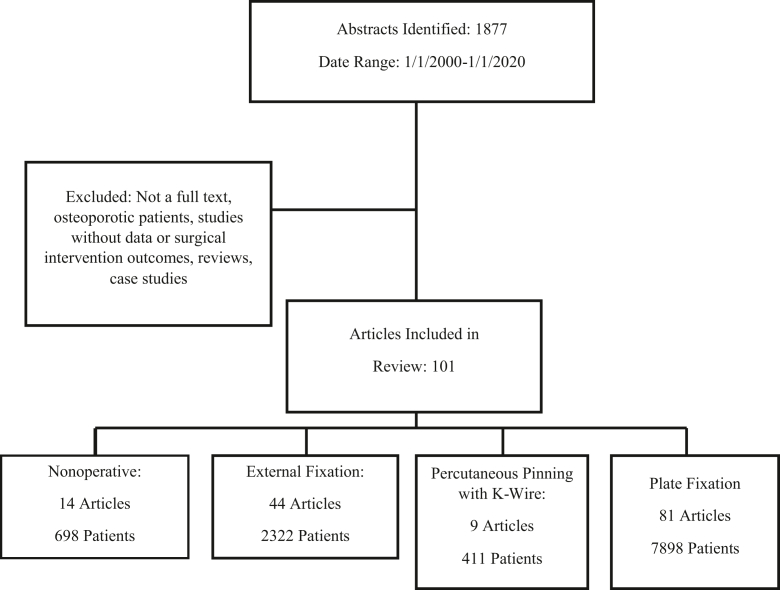
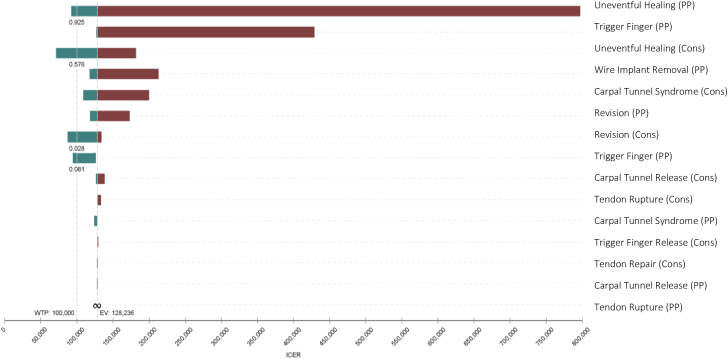
Methods: We created a decision tree to model the following treatment modalities for distal radius fractures: nonsurgical management, external fixation, percutaneous pinning, and plate fixation. Each node of the model was associated with specific costs in dollars, a utility adjustment (quality-adjusted life year [QALY]), and a percent likelihood. The nodes of the decision tree included uneventful healing, eventful healing and no further intervention, carpal tunnel syndrome, trigger finger, and tendon rupture as well as associated treatments for each event. The percent probabilities of each transition state, QALY values, and costs of intervention were gleaned from a systematic review. Rollback and incremental cost-effectiveness ratio analyses were conducted to identify optimal treatment strategies. Threshold values of $50,000/QALY and $100,000/QALY were used to distinguish the modalities in the incremental cost-effectiveness ratio analysis.
Results: Both the rollback analysis and the incremental cost-effectiveness ratio analysis revealed nonsurgical management as the predominant strategy when compared with the other operative modalities. Nonsurgical management dominated external fixation and plate fixation, although it was comparable with percutaneous fixation, yielding a $2,242 lesser cost and 0.017 lesser effectiveness.
Conclusions: The cost effectiveness of nonsurgical management is driven by its decreased cost to the health care system. Plate and external fixation have been shown to be both more expensive and less effective than other proposed treatments. Percutaneous pinning has demonstrated more favorable effectiveness in the literature than plate and external fixation and, thus, may be more cost effective in certain circumstances. Future studies may find value in investigating further clinical aspects of distal radius fractures and their association with nonsurgical management versus that with plate fixation.
Type of study/level of evidence: Economic/decision analysis II.
Keywords: Cost effectiveness; Distal radius fracture; Incremental cost-effectiveness ratio; Quality-adjusted life year; Rollback analysis.
© 2022 THE AUTHORS. Published by Elsevier Inc. on behalf of The American Society for Surgery of the Hand.
Figures
Similar articles
-
The Cost-Effectiveness of Surgical Fixation of Distal Radial Fractures: A Computer Model-Based Evaluation of Three Operative Modalities.J Bone Joint Surg Am. 2018 Feb 7;100(3):e13. doi: 10.2106/JBJS.17.00181. J Bone Joint Surg Am. 2018. PMID: 29406347 Free PMC article.
-
Neer Type-II Distal Clavicle Fractures: A Cost-Effectiveness Analysis of Fixation Techniques.J Bone Joint Surg Am. 2020 Feb 5;102(3):254-261. doi: 10.2106/JBJS.19.00590. J Bone Joint Surg Am. 2020. PMID: 31809393
-
Cost-Effectiveness of Volar Locking Plate Compared with Augmented External Fixation for Displaced Intra-Articular Wrist Fractures.J Bone Joint Surg Am. 2020 Dec 2;102(23):2049-2059. doi: 10.2106/JBJS.19.01288. J Bone Joint Surg Am. 2020. PMID: 32947595
-
Reverse Total Shoulder Arthroplasty Is the Most Cost-effective Treatment Strategy for Proximal Humerus Fractures in Older Adults: A Cost-utility Analysis.Clin Orthop Relat Res. 2022 Oct 1;480(10):2013-2026. doi: 10.1097/CORR.0000000000002219. Epub 2022 May 4. Clin Orthop Relat Res. 2022. PMID: 35507306 Free PMC article.
-
Rockwood Grade-III Acromioclavicular Joint Separation: A Cost-Effectiveness Analysis of Treatment Options.JB JS Open Access. 2021 May 4;6(2):e20.00171. doi: 10.2106/JBJS.OA.20.00171. eCollection 2021 Apr-Jun. JB JS Open Access. 2021. PMID: 34056509 Free PMC article.
Cited by
-
Surgical vs. Conservative Treatment of Distal Radius Fractures in the Elderly: A Systematic Review and Meta-Analysis.Cureus. 2024 Dec 17;16(12):e75879. doi: 10.7759/cureus.75879. eCollection 2024 Dec. Cureus. 2024. PMID: 39759677 Free PMC article. Review.
-
One week versus three to five weeks of plaster cast immobilization for nonreduced distal radius fractures, a cost effectiveness analysis embedded in a stepped wedge cluster randomized controlled trial.Eur J Health Econ. 2025 Jun 2. doi: 10.1007/s10198-025-01795-2. Online ahead of print. Eur J Health Econ. 2025. PMID: 40456952
References
-
- Karl J.W., Olson P.R., Rosenwasser M.P. The epidemiology of upper extremity fractures in the United States, 2009. J Orthop Trauma. 2015;29(8):e242–e244. - PubMed
-
- Shauver M.J., Yin H., Banerjee M., Chung K.C. Current and future national costs to medicare for the treatment of distal radius fracture in the elderly. J Hand Surg Am. 2011;36(8):1282–1287. - PubMed
-
- Mauck B.M., Swigler C.W. Evidence-based review of distal radius fractures. Orthop Clin North Am. 2018;49(2):211–222. - PubMed
-
- Stephens A.R., Presson A.P., McFarland M.M., et al. Volar locked plating versus closed reduction and casting for acute, displaced distal radial fractures in the elderly: a systematic review and meta-analysis of randomized controlled trials. J Bone Joint Surg Am. 2020;102(14):1280–1288. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
