

Approach to the Patient With Prolactinoma
- PMID: 36974474
- PMCID: PMC10438891
- DOI: 10.1210/clinem/dgad174
Approach to the Patient With Prolactinoma
Abstract
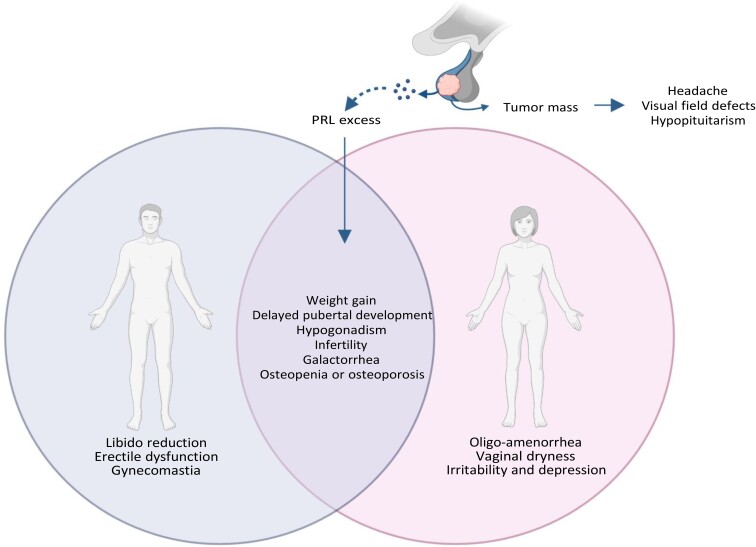
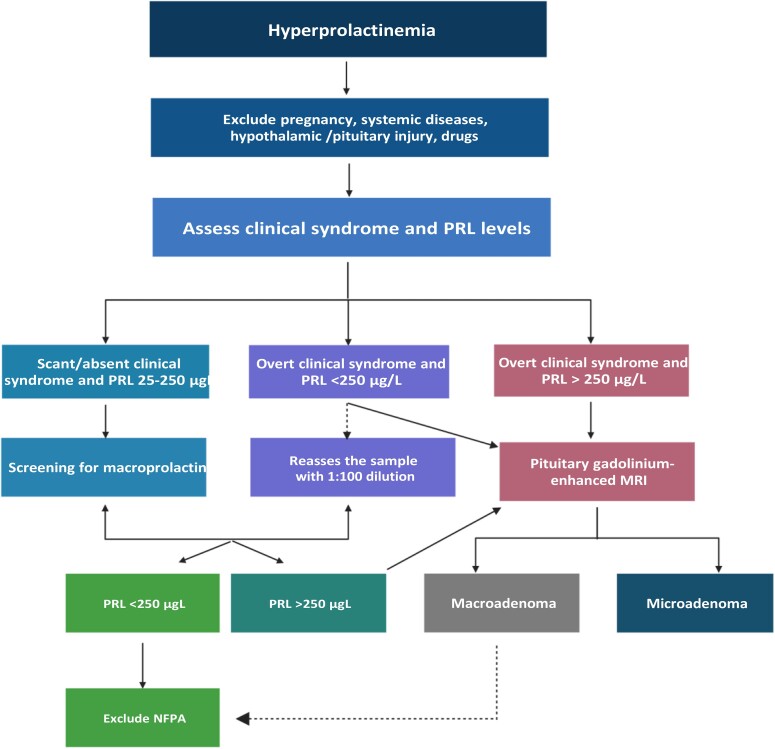
Prolactinomas are the most common pituitary tumor histotype, with microprolactinomas being prevalent in women and macroprolactinomas in men. Hyperprolactinemia is among the most common causes of hypogonadotropic hypogonadism in both sexes, prompting medical advice for hypogonadism (infertility, oligo-amenorrhea, impotence, osteoporosis/osteopenia) in both sexes, and for signs and symptoms of mass effects (hypopituitarism, visual loss, optic chiasm compression, cranial nerve deficits, headaches) predominantly in men. Diagnostic workup involves a single prolactin measurement and pituitary imaging, but some laboratory artifacts (ie, the "hook effect" and macroprolactin) can complicate or delay the diagnosis. The treatment of choice for prolactinomas is represented by dopamine agonists, mainly cabergoline, which are able to induce disease control, restore fertility in both sexes, and definitively cure one-third of patients, thus permitting treatment discontinuation. Pregnancy and menopause may promote spontaneous prolactin decline and anticipate cabergoline discontinuation in women. Surgery and/or radiotherapy are indicated in case of resistance to cabergoline not overcome by the increase in drug dose up to the maximally tolerated or the patient's personal choice of surgery. The evidence of resistance to cabergoline in invasive and proliferative tumors may indicate biological aggressiveness, thus requiring alternative therapeutic approaches mainly based on temozolomide use as monotherapy or combined with radiotherapy. In uncontrolled patients, new medical approaches (alternative hormonal treatments, cytotoxic drugs, peptide receptor radionuclide therapy, mTOR/Akt inhibitors, tyrosine kinase inhibitors, or immunotherapy) may be offered but the experience collected to date is still very scant. This article reviews different facets of prolactinomas and discusses approaches to the condition in more common clinical situations.
Keywords: cabergoline; dopamine agonists; hyperprolactinemia; menopause; pituitary tumor; pregnancy; prolactin; treatment withdrawal.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- De Lellis RA, Lloyd RV, Heitz PU, Eng C, Eng C, Machado De Avila RA. Pathology and Genetics of Tumours of Endocrine Organs. IARC Press; 2004.
-
- Gillam MP, Molitch ME, Lombardi G, Colao A. Advances in the treatment of prolactinomas. Endocr Rev. 2006;27(5):485‐534. - PubMed
-
- Colao A, Lombardi G. Growth-hormone and prolactin excess. Lancet. 1998;352(9138):1455‐1461. - PubMed
-
- Schlechte JA. Clinical practice prolactinoma. N Engl J Med. 2003;349(21):2035‐2041. - PubMed
-
- Cunnah D, Besser M. Management of prolactinomas. Clin Endocrinol. 1991;34(3):231‐235. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
