

Progression of atypical parkinsonian syndromes: PROSPECT-M-UK study implications for clinical trials
- PMID: 36975168
- PMCID: PMC10393398
- DOI: 10.1093/brain/awad105
Progression of atypical parkinsonian syndromes: PROSPECT-M-UK study implications for clinical trials
Abstract
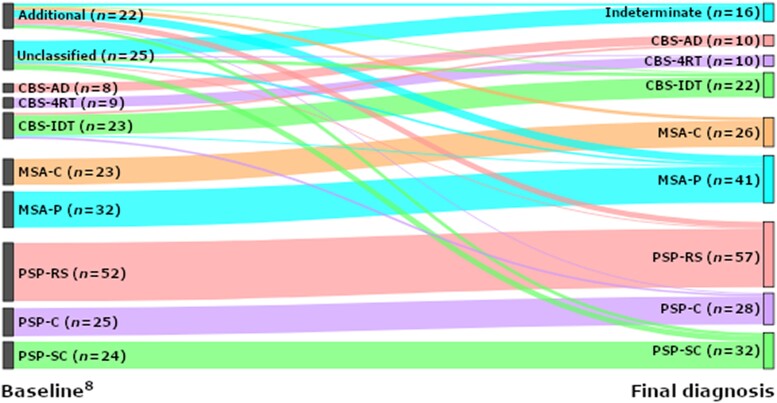
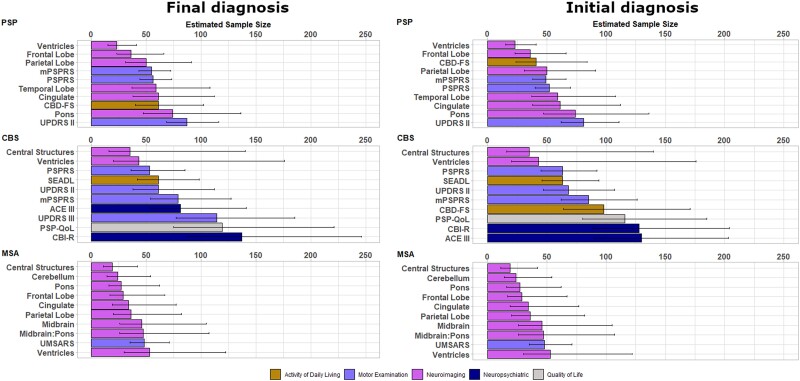
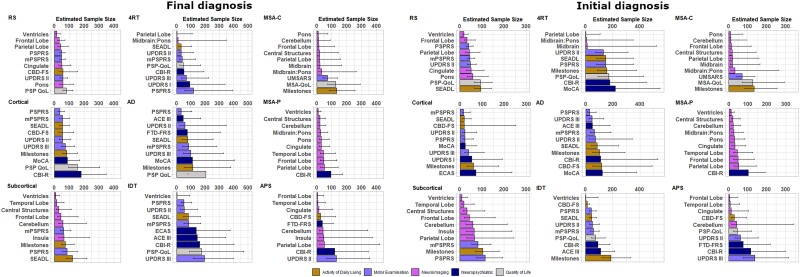
The advent of clinical trials of disease-modifying agents for neurodegenerative disease highlights the need for evidence-based end point selection. Here we report the longitudinal PROSPECT-M-UK study of progressive supranuclear palsy (PSP), corticobasal syndrome (CBS), multiple system atrophy (MSA) and related disorders, to compare candidate clinical trial end points. In this multicentre UK study, participants were assessed with serial questionnaires, motor examination, neuropsychiatric and MRI assessments at baseline, 6 and 12 months. Participants were classified by diagnosis at baseline and study end, into Richardson syndrome, PSP-subcortical (PSP-parkinsonism and progressive gait freezing subtypes), PSP-cortical (PSP-frontal, PSP-speech and language and PSP-CBS subtypes), MSA-parkinsonism, MSA-cerebellar, CBS with and without evidence of Alzheimer's disease pathology and indeterminate syndromes. We calculated annual rate of change, with linear mixed modelling and sample sizes for clinical trials of disease-modifying agents, according to group and assessment type. Two hundred forty-three people were recruited [117 PSP, 68 CBS, 42 MSA and 16 indeterminate; 138 (56.8%) male; age at recruitment 68.7 ± 8.61 years]. One hundred and fifty-nine completed the 6-month assessment (82 PSP, 27 CBS, 40 MSA and 10 indeterminate) and 153 completed the 12-month assessment (80 PSP, 29 CBS, 35 MSA and nine indeterminate). Questionnaire, motor examination, neuropsychiatric and neuroimaging measures declined in all groups, with differences in longitudinal change between groups. Neuroimaging metrics would enable lower sample sizes to achieve equivalent power for clinical trials than cognitive and functional measures, often achieving N < 100 required for 1-year two-arm trials (with 80% power to detect 50% slowing). However, optimal outcome measures were disease-specific. In conclusion, phenotypic variance within PSP, CBS and MSA is a major challenge to clinical trial design. Our findings provide an evidence base for selection of clinical trial end points, from potential functional, cognitive, clinical or neuroimaging measures of disease progression.
Keywords: clinical trials; corticobasal syndrome; multiple system atrophy; progressive supranuclear palsy; sample size.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
H.Z. has served at scientific advisory boards and/or as a consultant for Abbvie, Alector, Annexon, Artery Therapeutics, AZTherapies, CogRx, Denali, Eisai, Nervgen, Pinteon Therapeutics, Red Abbey Labs, Passage Bio, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, Biogen, and Roche, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). N.P. has received consultancy fees and speaker fees from Bial, AbbVie, Roche, 4D Pharma, Britannia. M.H. has received funding/grant support from Parkinson’s UK, Oxford NIHR BRC, University of Oxford, CPT, Lab10X, NIHR, Michael J Fox Foundation, H2020 European Union, GE Healthcare and the PSP Association. She also received payment for Advisory Board attendance/consultancy for Biogen, Roche, Sanofi Aventis, CuraSen Therapeutics, Evidera, Manus Neurodynamica, Lundbeck. H.M. is employed by UCL. In the last 12 months he reports paid consultancy from Roche and Amylyx; lecture fees/honoraria—BMJ, Kyowa Kirin, Movement Disorders Society. Research Grants from Parkinson’s UK, Cure Parkinson’s Trust, PSP Association, Medical Research Council, Michael J Fox Foundation. H.M. is a co-applicant on a patent application related to C9ORF72—Method for diagnosing a neurodegenerative disease (PCT/GB2012/052140).
J.B.R. has research grants unrelated to the current work from AstraZeneca, Janssen, Lilly, GSK via the Dementias Platform UK; and has provided consultancy unrelated to the current work, to Asceneuron, Astex, Curasen, UCB, SV Health, WAVE and Alzheimer Research UK. All other authors report no competing interests related to this work.
The sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Figures
References
-
- Schrag A, Ben-Shlomo Y, Quinn NP. Prevalence of progressive supranuclear palsy and multiple system atrophy: A cross-sectional study. Lancet. 1999;354:1771–1775. - PubMed
-
- Nath U. The prevalence of progressive supranuclear palsy (steele-richardson-olszewski syndrome) in the UK. Brain. 2001;124:1438–1449. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
