

CAPER: patient preferences to inform nonsurgical treatment of chronic low back pain: a discrete-choice experiment
- PMID: 36975607
- PMCID: PMC12394812
- DOI: 10.1093/pm/pnad038
CAPER: patient preferences to inform nonsurgical treatment of chronic low back pain: a discrete-choice experiment
Abstract
Objective: We developed and used a discrete-choice measure to study patient preferences with regard to the risks and benefits of nonsurgical treatments when they are making treatment selections for chronic low back pain.
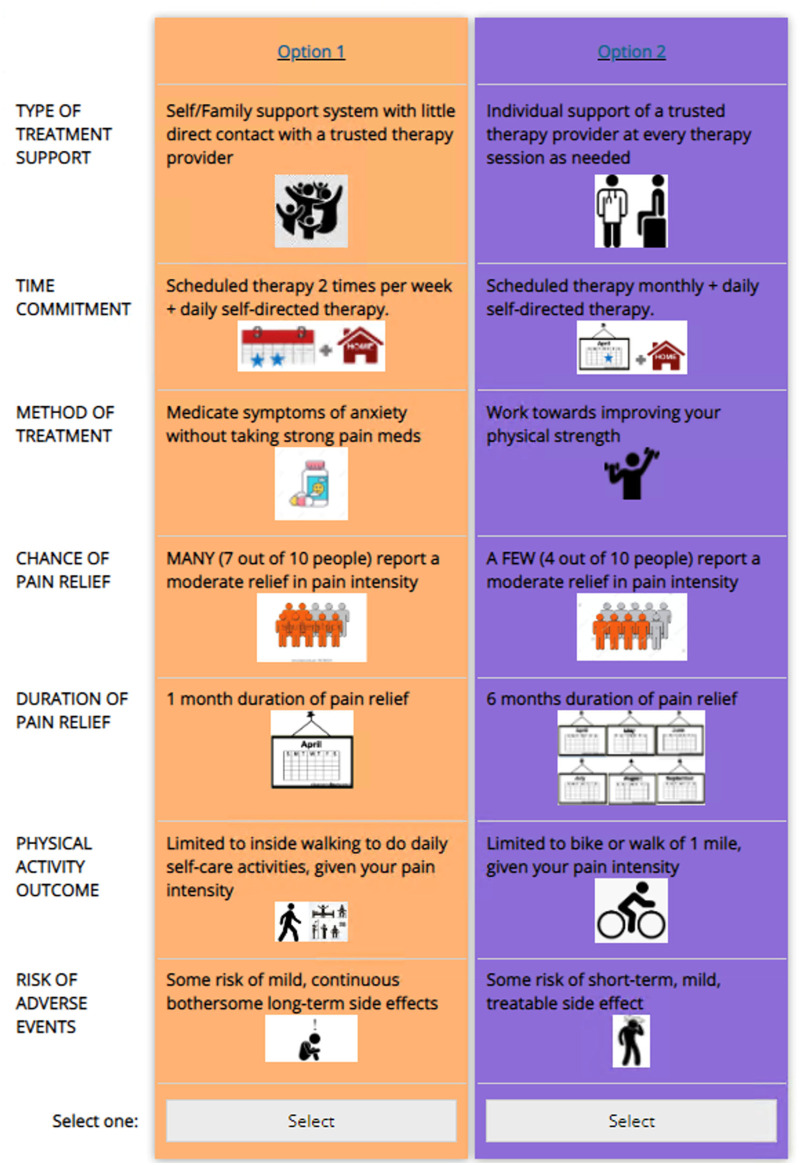
Methods: "CAPER TREATMENT" (Leslie Wilson) was developed with standard choice-based conjoint procedures (discrete-choice methodology that mimics an individual's decision-making process). After expert input and pilot testing, our final measure had 7 attributes (chance of pain relief, duration of relief, physical activity changes, treatment method, treatment type, treatment time burden, and risks of treatment) with 3-4 levels each. Using Sawtooth software (Sawtooth Software, Inc., Provo, UT, USA), we created a random, full-profile, balanced-overlap experimental design. Respondents (n = 211) were recruited via an emailed online link and completed 14 choice-based conjoint choice pairs; 2 fixed questions; and demographic, clinical, and quality-of-life questions. Analysis was performed with random-parameters multinomial logit with 1000 Halton draws.
Results: Patients cared most about the chance of pain relief, followed closely by improving physical activity, even more than duration of pain relief. There was comparatively less concern about time commitment and risks. Gender and socioeconomic status influenced preferences, especially with relation to strength of expectations for outcomes. Patients experiencing a low level of pain (Pain, Enjoyment, and General Activity Scale [PEG], question 1, numeric rating scale score<4) had a stronger desire for maximally improved physical activity, whereas those in a high level of pain (PEG, question 1, numeric rating scale score>6) preferred both maximum and more limited activity. Highly disabled patients (Oswestry Disability Index score>40) demonstrated distinctly different preferences, placing more weight on achieving pain control and less on improving physical activity.
Conclusions: Individuals with chronic low back pain were willing to trade risks and inconveniences for better pain control and physical activity. Additionally, different preference phenotypes exist, which suggests a need for clinicians to target treatments to particular patients.
Keywords: choice-based conjoint; chronic low back pain; chronic low back pain treatment; decision-making; discrete-choice experiment; pain; patient preference.
© The Author(s) 2023. Published by Oxford University Press on behalf of the American Academy of Pain Medicine. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures




References
-
- Gooch CL, Pracht E, Borenstein AR.. The burden of neurological disease in the United States: a summary report and call to action. Ann Neurol. 2017;81(4):479-484. - PubMed
-
- Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP.. Low back pain. Lancet. 2021;398:78–92. - PubMed
-
- U.S. Food and Drug Administration. List of Patient Preference-Sensitive Priority Areas. Accessed June 27, 2021. https://www.fda.gov/about-fda/cdrh-patient-science-and-engagement-progra....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
