

Genomic Characterization of Carbapenem-Resistant Acinetobacter baumannii (CRAB) in Mechanically Ventilated COVID-19 Patients and Impact of Infection Control Measures on Reducing CRAB Circulation during the Second Wave of the SARS-CoV-2 Pandemic in Milan, Italy
- PMID: 36976013
- PMCID: PMC10100775
- DOI: 10.1128/spectrum.00209-23
Genomic Characterization of Carbapenem-Resistant Acinetobacter baumannii (CRAB) in Mechanically Ventilated COVID-19 Patients and Impact of Infection Control Measures on Reducing CRAB Circulation during the Second Wave of the SARS-CoV-2 Pandemic in Milan, Italy
Abstract
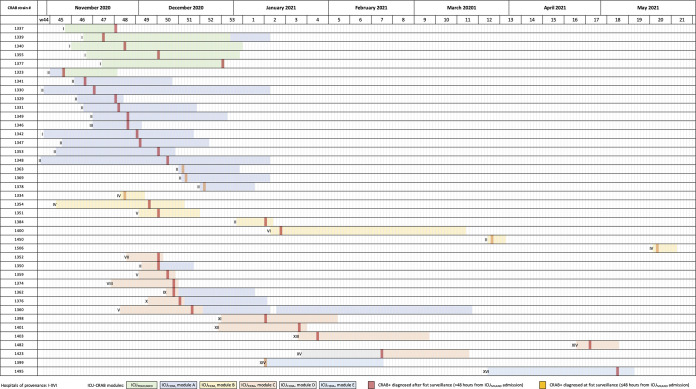
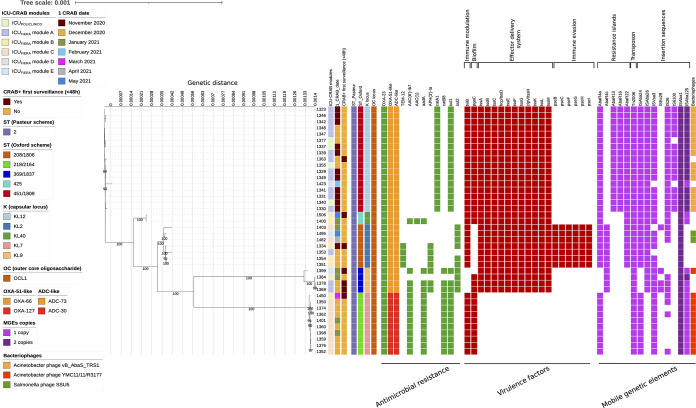
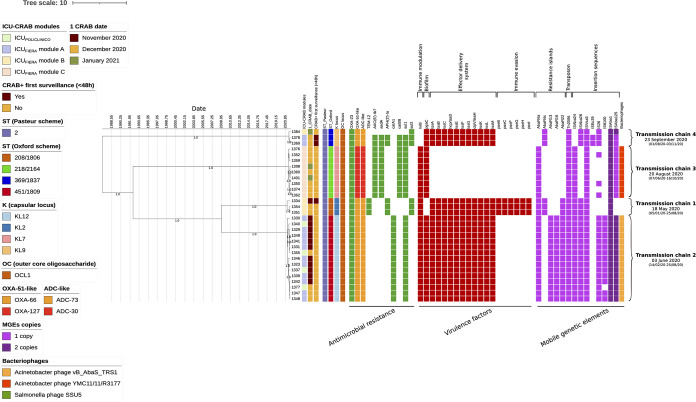
COVID-19 has significantly affected hospital infection prevention and control (IPC) practices, especially in intensive care units (ICUs). This frequently caused dissemination of multidrug-resistant organisms (MDROs), including carbapenem-resistant Acinetobacter baumannii (CRAB). Here, we report the management of a CRAB outbreak in a large ICU COVID-19 hub Hospital in Italy, together with retrospective genotypic analysis by whole-genome sequencing (WGS). Bacterial strains obtained from severe COVID-19 mechanically ventilated patients diagnosed with CRAB infection or colonization between October 2020 and May 2021 were analyzed by WGS to assess antimicrobial resistance and virulence genes, along with mobile genetic elements. Phylogenetic analysis in combination with epidemiological data was used to identify putative transmission chains. CRAB infections and colonization were diagnosed in 14/40 (35%) and 26/40 (65%) cases, respectively, with isolation within 48 h from admission in 7 cases (17.5%). All CRAB strains belonged to Pasteur sequence type 2 (ST2) and 5 different Oxford STs and presented blaOXA-23 gene-carrying Tn2006 transposons. Phylogenetic analysis revealed the existence of four transmission chains inside and among ICUs, circulating mainly between November and January 2021. A tailored IPC strategy was composed of a 5-point bundle, including ICU modules' temporary conversion to CRAB-ICUs and dynamic reopening, with limited impact on ICU admission rate. After its implementation, no CRAB transmission chains were detected. Our study underlies the potentiality of integrating classical epidemiological studies with genomic investigation to identify transmission routes during outbreaks, which could represent a valuable tool to ensure IPC strategies and prevent the spread of MDROs. IMPORTANCE Infection prevention and control (IPC) practices are of paramount importance for preventing the spread of multidrug-resistant organisms (MDROs) in hospitals, especially in the intensive care unit (ICU). Whole-genome sequencing (WGS) is seen as a promising tool for IPC, but its employment is currently still limited. COVID-19 pandemics have posed dramatic challenges in IPC practices, causing worldwide several outbreaks of MDROs, including carbapenem-resistant Acinetobacter baumannii (CRAB). We present the management of a CRAB outbreak in a large ICU COVID-19 hub hospital in Italy using a tailored IPC strategy that allowed us to contain CRAB transmission while preventing ICU closure during a critical pandemic period. The analysis of clinical and epidemiological data coupled with retrospective genotypic analysis by WGS identified different putative transmission chains and confirmed the effectiveness of the IPC strategy implemented. This could be a promising approach for future IPC strategies.
Keywords: Acinetobacter baumannii CRAB; genomic surveillance; infection prevention and control (IPC); intensive care unit (ICU); phylogenetic analysis; whole-genome sequencing (WGS).
Conflict of interest statement
The authors declare a conflict of interest. Giacomo Grasselli reported: - payment for lectures from Pfizer, MSD, Mundipharma - unrestricted research grants from Pfizer and MSD - advisory board participation: Glaxo Smith Klein. Claudia Alteri acknowledges fees for lectures from Pfizer.
Figures
References
-
- Vincent J-L, Sakr Y, Singer M, Martin-Loeches I, Machado FR, Marshall JC, Finfer S, Pelosi P, Brazzi L, Aditianingsih D, Timsit J-F, Du B, Wittebole X, Máca J, Kannan S, Gorordo-Delsol LA, De Waele JJ, Mehta Y, Bonten MJM, Khanna AK, Kollef M, Human M, Angus DC, EPIC III Investigators . 2020. Prevalence and outcomes of infection among patients in intensive care units in 2017. JAMA 323:1478–1487. doi: 10.1001/jama.2020.2717. - DOI - PMC - PubMed
-
- Martín-Aspas A, Guerrero-Sánchez FM, García-Colchero F, Rodríguez-Roca S, Girón-González JA. 2018. Differential characteristics of Acinetobacter baumannii colonization and infection: risk factors, clinical picture, and mortality. Infect Drug Resist 11:861–872. doi: 10.2147/IDR.S163944. - DOI - PMC - PubMed
-
- Garnacho-Montero J, Gutiérrez-Pizarraya A, Díaz-Martín A, Cisneros-Herreros JM, Cano ME, Gato E, Ruiz de Alegría C, Fernández-Cuenca F, Vila J, Martínez-Martínez L, Tomás-Carmona MDM, Pascual Á, Bou G, Pachón-Diaz J, Rodríguez-Baño J. 2016. Acinetobacter baumannii in critically ill patients: molecular epidemiology, clinical features and predictors of mortality. Enferm Infecc Microbiol Clin 34:551–558. doi: 10.1016/j.eimc.2015.11.018. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
