

Pharmacologic improvement of CFTR function rapidly decreases sputum pathogen density, but lung infections generally persist
- PMID: 36976651
- PMCID: PMC10178839
- DOI: 10.1172/JCI167957
Pharmacologic improvement of CFTR function rapidly decreases sputum pathogen density, but lung infections generally persist
Abstract
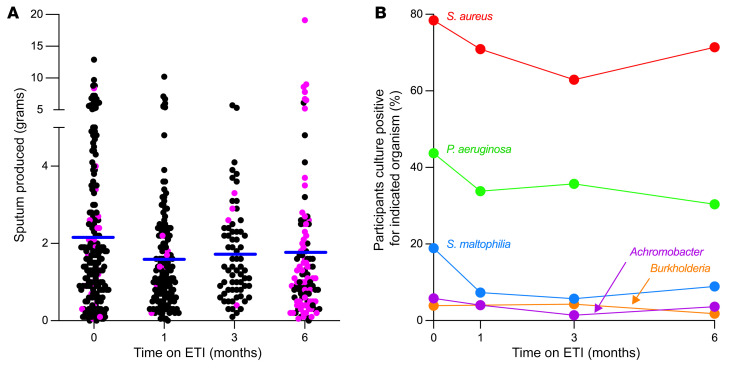
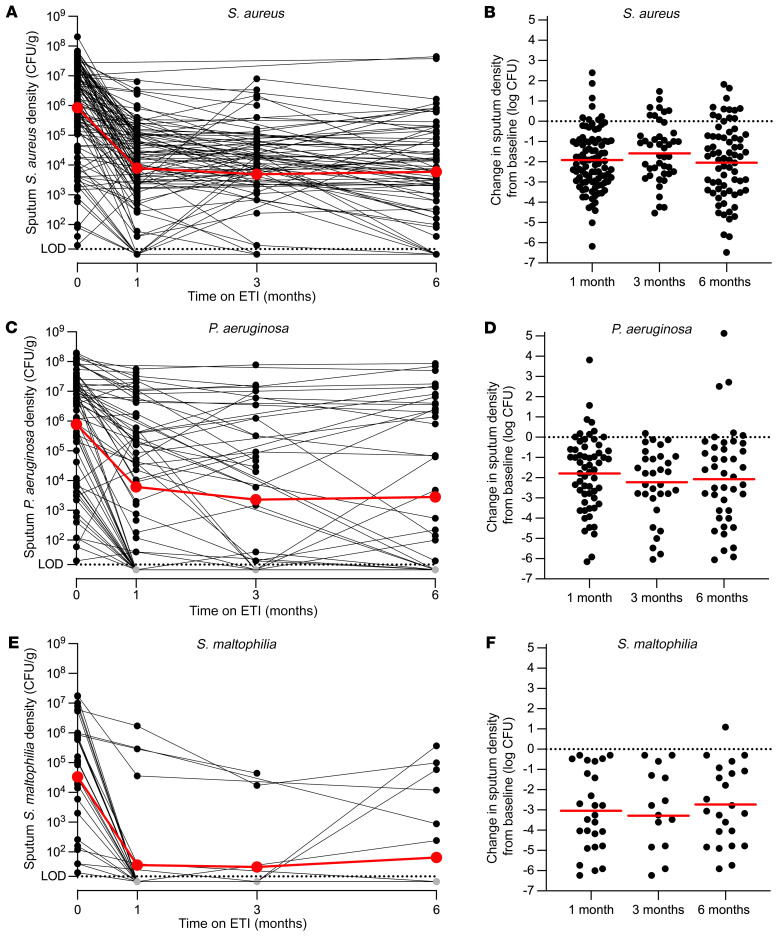
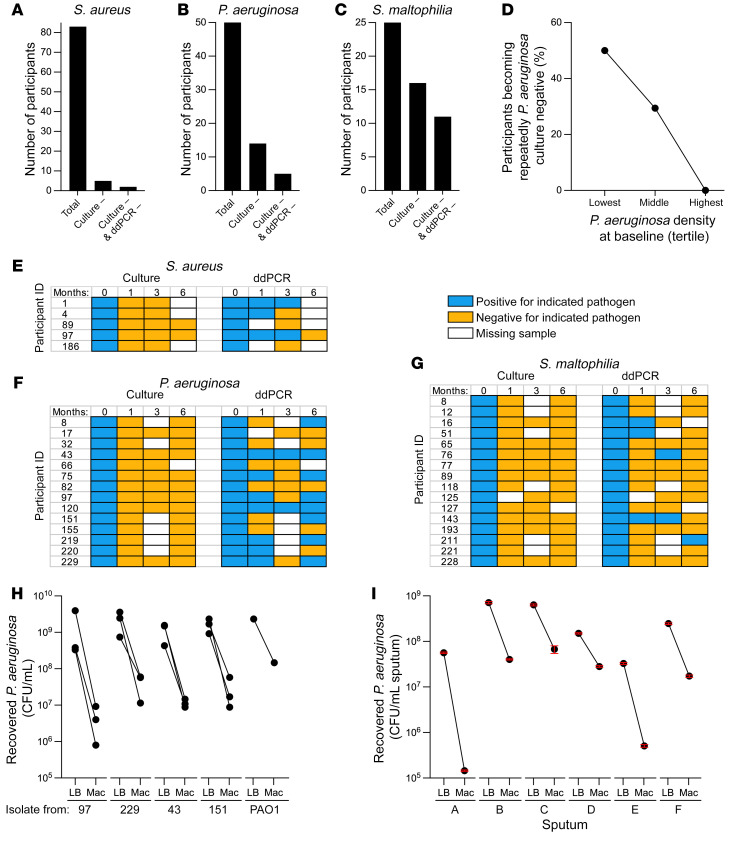
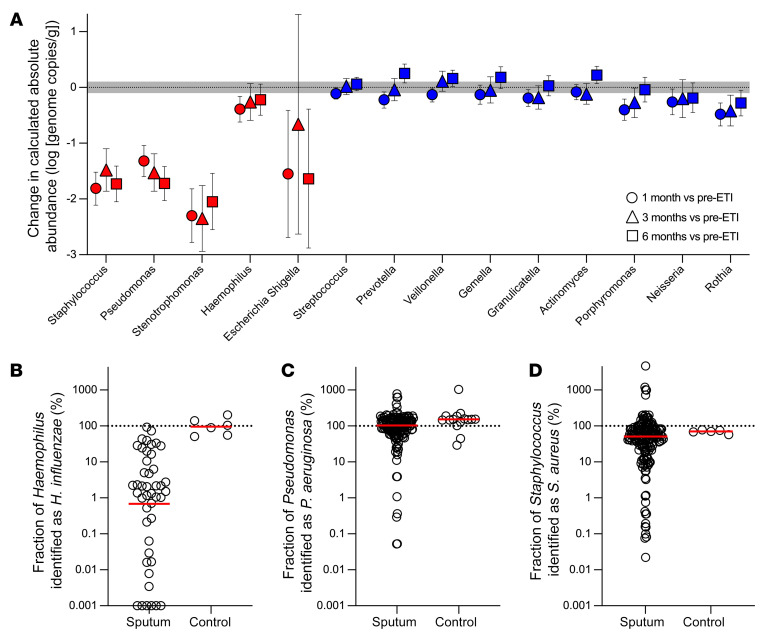
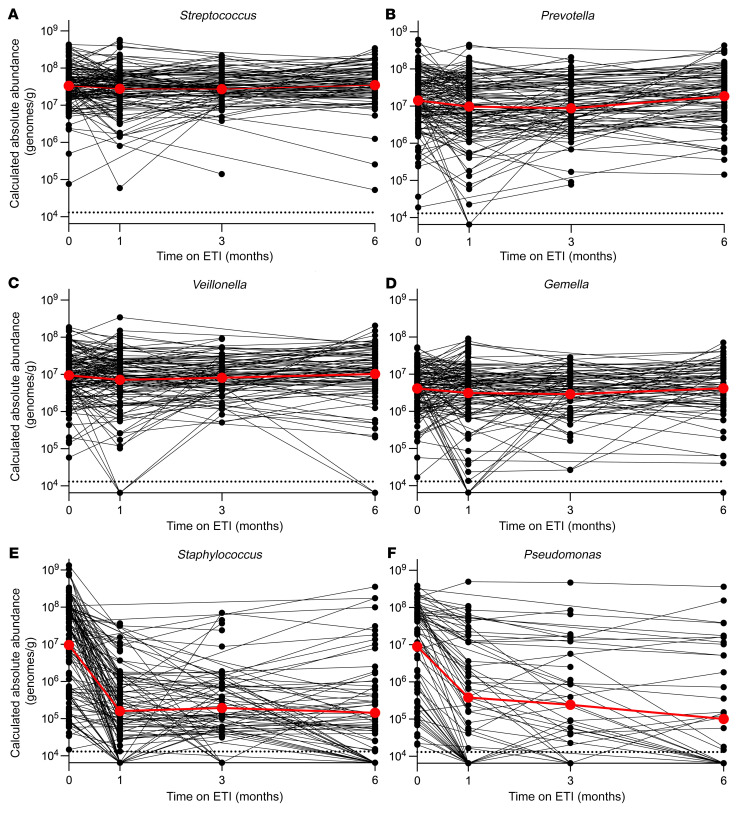
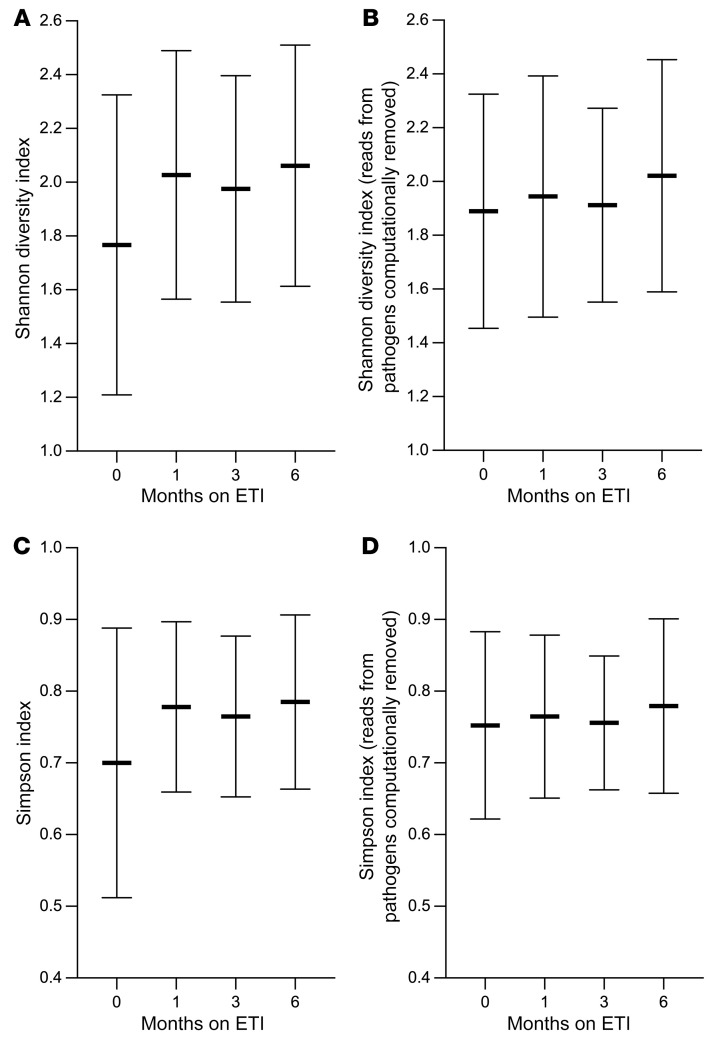
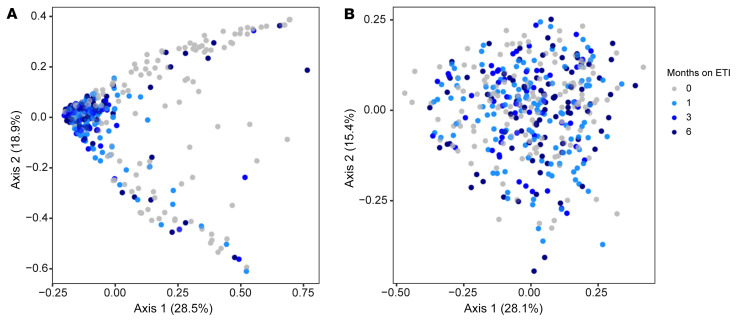
BackgroundLung infections are among the most consequential manifestations of cystic fibrosis (CF) and are associated with reduced lung function and shortened survival. Drugs called CF transmembrane conductance regulator (CFTR) modulators improve activity of dysfunctional CFTR channels, which is the physiological defect causing CF. However, it is unclear how improved CFTR activity affects CF lung infections.MethodsWe performed a prospective, multicenter, observational study to measure the effect of the newest and most effective CFTR modulator, elexacaftor/tezacaftor/ivacaftor (ETI), on CF lung infections. We studied sputum from 236 people with CF during their first 6 months of ETI using bacterial cultures, PCR, and sequencing.ResultsMean sputum densities of Staphylococcus aureus, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, Achromobacter spp., and Burkholderia spp. decreased by 2-3 log10 CFU/mL after 1 month of ETI. However, most participants remained culture positive for the pathogens cultured from their sputum before starting ETI. In those becoming culture negative after ETI, the pathogens present before treatment were often still detectable by PCR months after sputum converted to culture negative. Sequence-based analyses confirmed large reductions in CF pathogen genera, but other bacteria detected in sputum were largely unchanged. ETI treatment increased average sputum bacterial diversity and produced consistent shifts in sputum bacterial composition. However, these changes were caused by ETI-mediated decreases in CF pathogen abundance rather than changes in other bacteria.ConclusionsTreatment with the most effective CFTR modulator currently available produced large and rapid reductions in traditional CF pathogens in sputum, but most participants remain infected with the pathogens present before modulator treatment.Trial RegistrationClinicalTrials.gov NCT04038047.FundingThe Cystic Fibrosis Foundation and the NIH.
Keywords: Bacterial infections; Microbiology; Pulmonology.
Conflict of interest statement
Figures
References
-
- Heijerman HGM, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet. 2019;394(10212):1940–1948. doi: 10.1016/S0140-6736(19)32597-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
