

Effects of a Province-wide Triaging System for TIA: The ASPIRE Intervention
- PMID: 36977597
- PMCID: PMC10186240
- DOI: 10.1212/WNL.0000000000207201
Effects of a Province-wide Triaging System for TIA: The ASPIRE Intervention
Abstract
Background and objectives: Urgent transient ischemic attack (TIA) management to reduce stroke recurrence is challenging, particularly in rural and remote areas. In Alberta, Canada, despite an organized stroke system, data from 1999 to 2000 suggested that stroke recurrence after TIA was as high as 9.5% at 90 days. Our objective was to determine whether a multifaceted population-based intervention resulted in a reduction in recurrent stroke after TIA.
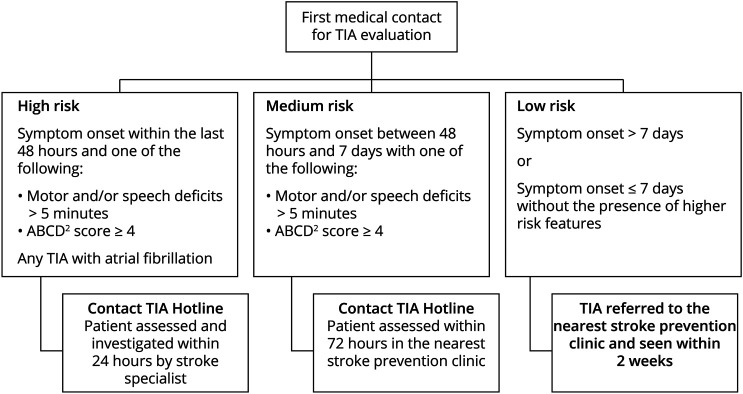
Methods: In this quasi-experimental health services research intervention study, we implemented a TIA management algorithm across the entire province, centered around a 24-hour physician's TIA hotline and public and health provider education on TIA. From administrative databases, we linked emergency department discharge abstracts to hospital discharge abstracts to identify incident TIAs and recurrent strokes at 90 days across a single payer system with validation of recurrent stroke events. The primary outcome was recurrent stroke; with a secondary composite outcome of recurrent stroke, acute coronary syndrome, and all-cause death. We used an interrupted time series regression analysis of age-adjusted and sex-adjusted stroke recurrence rates after TIA, incorporating a 2-year preimplementation period (2007-2009), a 15-month implementation period, and a 2-year postimplementation period (2010-2012). Logistic regression was used to examine outcomes that did not fit the time series model.
Results: We assessed 6,715 patients preimplementation and 6,956 patients postimplementation. The 90-day stroke recurrence rate in the pre-Alberta Stroke Prevention in TIA and mild Strokes (ASPIRE) period was 4.5% compared with 5.3% during the post-ASPIRE period. There was neither a step change (estimate 0.38; p = 0.65) nor slope change (parameter estimate 0.30; p = 0.12) in recurrent stroke rates associated with the ASPIRE intervention implementation period. Adjusted all-cause mortality (odds ratio 0.71, 95% CI 0.56-0.89) was significantly lower after the ASPIRE intervention.
Discussion: The ASPIRE TIA triaging and management interventions did not further reduce stroke recurrence in the context of an organized stroke system. The apparent lower mortality postintervention may be related to improved surveillance after events identified as TIAs, but secular trends cannot be excluded.
Classification of evidence: This study provides Class III evidence that a standardized population-wide algorithmic triage system for patients with TIA did not reduce recurrent stroke rate.
© 2023 American Academy of Neurology.
Conflict of interest statement
T.J. Jeerakathil received funding for this project from the Heart and Stroke Foundation of Canada, the Canadian Institutes for Health Research, and the Canadian Stroke Network. The TIA hotline component was funded by Alberta Health Services. A.Y.X. Yu received fellowship funding from Alberta Innovates Health Solutions. P.M.C. Choi, S. Fang, A. Shuaib, S.R. Majumdar, A.M. Demchuk, K.S. Butcher, T.J. Watson, N. Dean, D. Gordon, M.D. Hill, and C. Edmond reports no disclosures relevant to the manuscript. S.B. Coutts received funding for this project from the Heart and Stroke Foundation of Canada, the Canadian Institutes for Health Research, and the Canadian Stroke Network. The TIA hotline component was funded by Alberta Health Services. S.B> Coutts received salary support from the Alberta Innovates-Health solutions and the Heart and Stroke Foundation of Canada's Distinguished Clinician Scientist award, supported in partnership with the Canadian Institute of Health Research (CIHR), Institute of Circulatory and Respiratory Health, and AstraZeneca Canada Inc. Go to
Figures

References
-
- Rothwell PM, Warlow CP. Timing of TIAs preceding stroke: time window for prevention is very short. Neurology. 2005;64(5):817-820. - PubMed
-
- Johnston SC, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284(22):2901-2906. - PubMed
-
- Hill MD, Yiannakoulias N, Jeerakathil T, Tu JV, Svenson LW, Schopflocher DP. The high risk of stroke immediately after transient ischemic attack: a population-based study. Neurology. 2004;62(11):2015-2020. - PubMed
-
- Kleindorfer D, Panagos P, Pancioli A, et al. Incidence and short-term prognosis of transient ischemic attack in a population-based study. Stroke. 2005;36(4):720-723. - PubMed
-
- Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370(9596):1432-1442. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials