

Computed Tomography Bronchus Sign Subclassification during Radial Endobronchial Ultrasound-Guided Transbronchial Biopsy: A Retrospective Analysis
- PMID: 36980372
- PMCID: PMC10047045
- DOI: 10.3390/diagnostics13061064
Computed Tomography Bronchus Sign Subclassification during Radial Endobronchial Ultrasound-Guided Transbronchial Biopsy: A Retrospective Analysis
Abstract
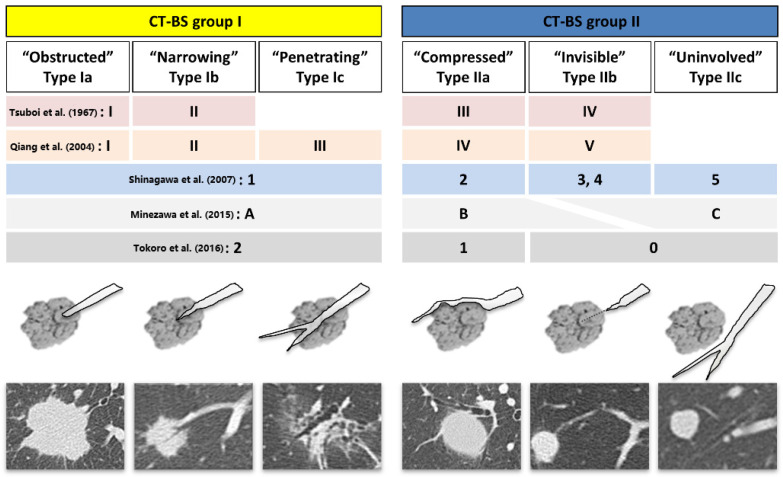
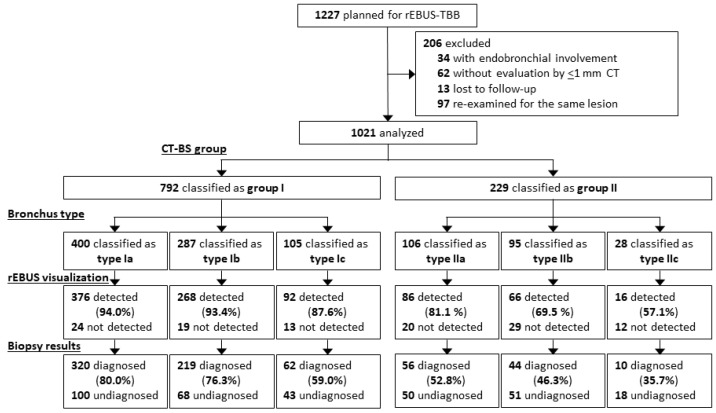
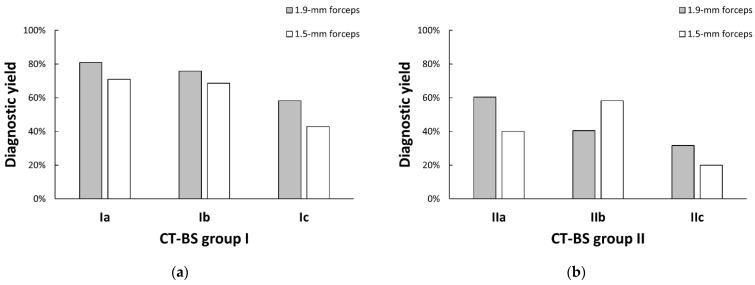
The presence of computed tomography bronchus sign (CT-BS) substantially increases the diagnostic yield of peripheral pulmonary lesions. However, the clinical significance of subdividing CT-BS remains controversial. We classified bronchus types on CT into six subtypes (CT-BS group I: types Ia-Ic with the bronchus connected within the lesion, group II: types IIa-IIc without connection) to clarify the differences in their characteristics and investigate the factors associated with diagnosis during radial endobronchial ultrasound (rEBUS)-guided bronchoscopy. In total, 1021 cases were analyzed. Our findings in diagnostic yields were that in CT-BS group I, penetrating type Ic was inferior to obstructed type Ia and narrowing type Ib (59.0% vs. 80.0% and 76.3%, p < 0.001, p = 0.004); in CT-BS group II, compressed type IIa showed no difference when compared with invisible type IIb and uninvolved type IIc (IIa: 52.8% vs. IIb: 46.3% and IIc: 35.7%, p = 0.253). Multivariable analysis revealed that bronchus type (types Ia and Ib vs. Ic) was a significant independent predictor of successful diagnosis in CT-BS group I (odds ratio, 1.78; 95% confidence interval, 1.04-3.05; p = 0.035), along with known factors such as rEBUS visualization. CT-BS subclassification may provide useful information regarding the bronchoscopic technique to facilitate accurate diagnosis.
Keywords: bronchoscopy; bronchus sign; lung cancer; peripheral pulmonary lesion; radial endobronchial ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- National Lung Screening Trial Research Team. Aberle D.R., Adams A.M., Berg C.D., Black W.C., Clapp J.D., Fagerstrom R.M., Gareen I.F., Gatsonis C., Marcus P.M., et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011;365:395–409. doi: 10.1056/NEJMoa1102873. - DOI - PMC - PubMed
-
- Ishida T., Asano F., Yamazaki K., Shinagawa N., Oizumi S., Moriya H., Munakata M., Nishimura M. Virtual Navigation in Japan Trial Group. Virtual bronchoscopic navigation combined with endobronchial ultrasound to diagnose small peripheral pulmonary lesions: A randomised trial. Thorax. 2011;66:1072–1077. doi: 10.1136/thx.2010.145490. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
