

Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker
- PMID: 36980435
- PMCID: PMC10047450
- DOI: 10.3390/diagnostics13061127
Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker
Abstract
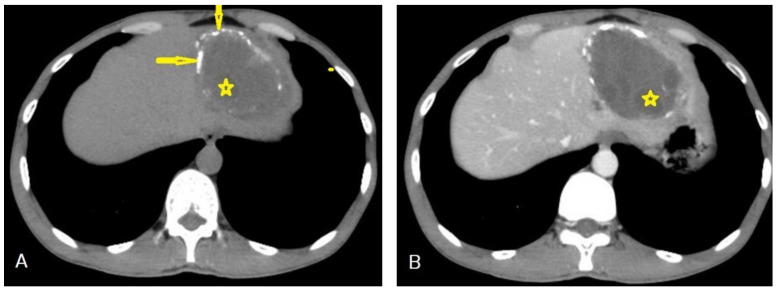
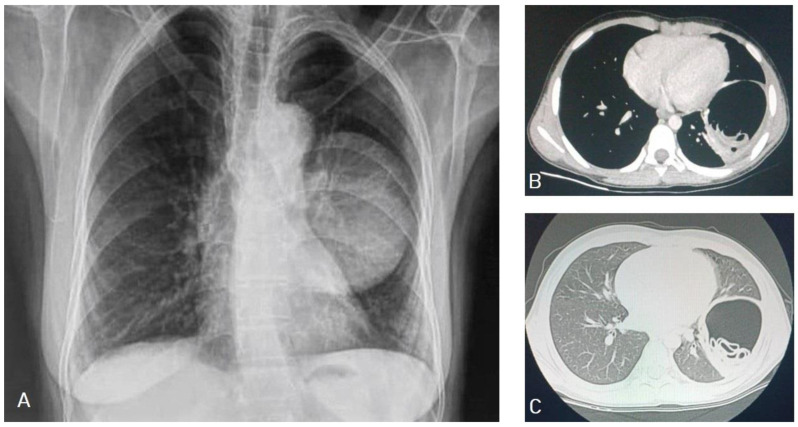
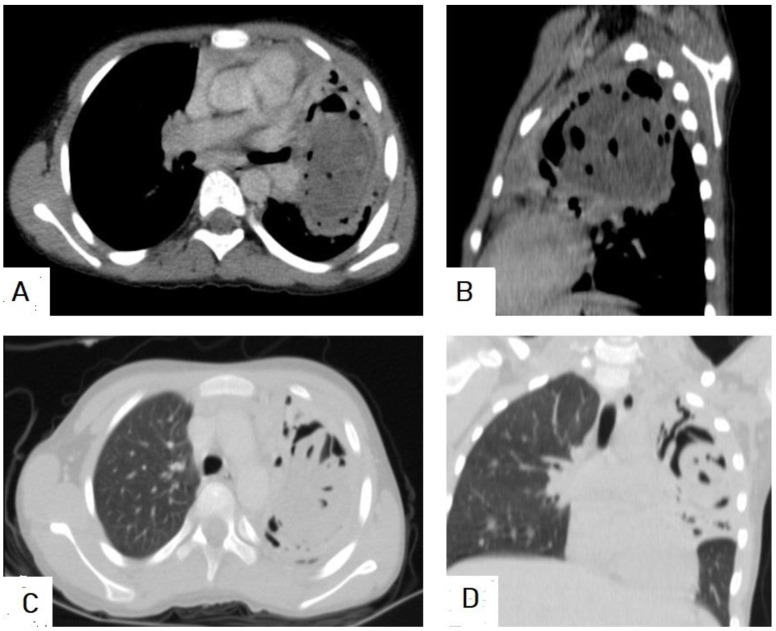
Hydatid cyst is a common name for the larval stage of a tapeworm species of Echinococcus granulosus, which is transmitted from animals to humans via the fecal-oral route. Hydatid cysts predominantly affect the liver (75%), followed by the lung (15%), and they can affect many organs in the human body. Medical imaging modalities are the keystone for the diagnosis of hydatid cysts with high sensitivity and specificity. Ultrasound imaging with high resolution is the first choice for diagnosis, differential diagnosis, staging, establishing a role in interventional management, and follow-up, and it can differentiate Type I hydatid cysts from simple liver cysts. Unenhanced computed tomography (CT) is indicated where or when an ultrasound is unsatisfactory, such as with chest or brain hydatid cysts, when detecting calcification, and in obese patients. Magnetic resonance imaging (MRI) is superior for demonstrating cyst wall defects, biliary communication, neural involvement, and differentiating hydatid cysts from simple cysts using diffusion-weighted imaging (DWI) sequences. According to the phase of growth, hydatid cysts occur in different sizes and shapes, which may mimic benign or malignant neoplasms and may create diagnostic challenges in some cases. Hydatid cysts can mimic simple cysts, choledochal cysts, Caroli's disease, or mesenchymal hamartomas of the liver. They can mimic lung cystic lesions, mycetoma, blood clots, Rasmussen aneurysms, and even lung carcinomas. Differential diagnosis can be difficult for arachnoid cysts, porencephalic cysts, pyogenic abscesses, and even cystic tumors of the brain, and can create diagnostic dilemmas in the musculoskeletal system.
Keywords: calcified cyst; cyst with daughter cysts; cyst with floating membranes; cyst with waterlily sign; larval stage of Echinococcus granulosus; spoke-wheel appearance; unilocular simple cyst.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






















References
-
- Torgerson P.R., Devleesschauwer B., Praet N., Speybroeck N., Willingham A.L., Kasuga F., Rokni M.B., Zhou X.N., Fèvre E.M., Sripa B., et al. World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis. PLoS Med. 2015;12:e1001920. doi: 10.1371/journal.pmed.1001920. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
