

Classification of Chondrosarcoma: From Characteristic to Challenging Imaging Findings
- PMID: 36980590
- PMCID: PMC10046282
- DOI: 10.3390/cancers15061703
Classification of Chondrosarcoma: From Characteristic to Challenging Imaging Findings
Abstract
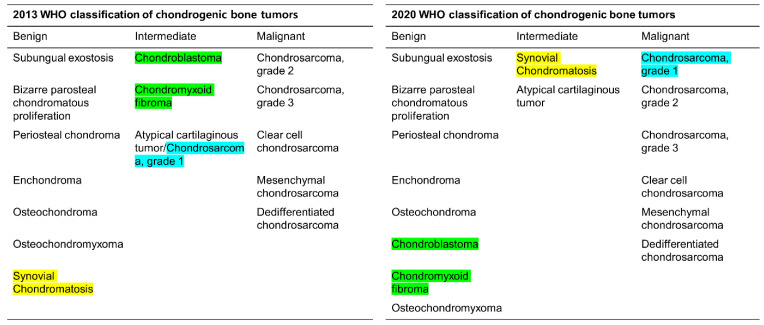
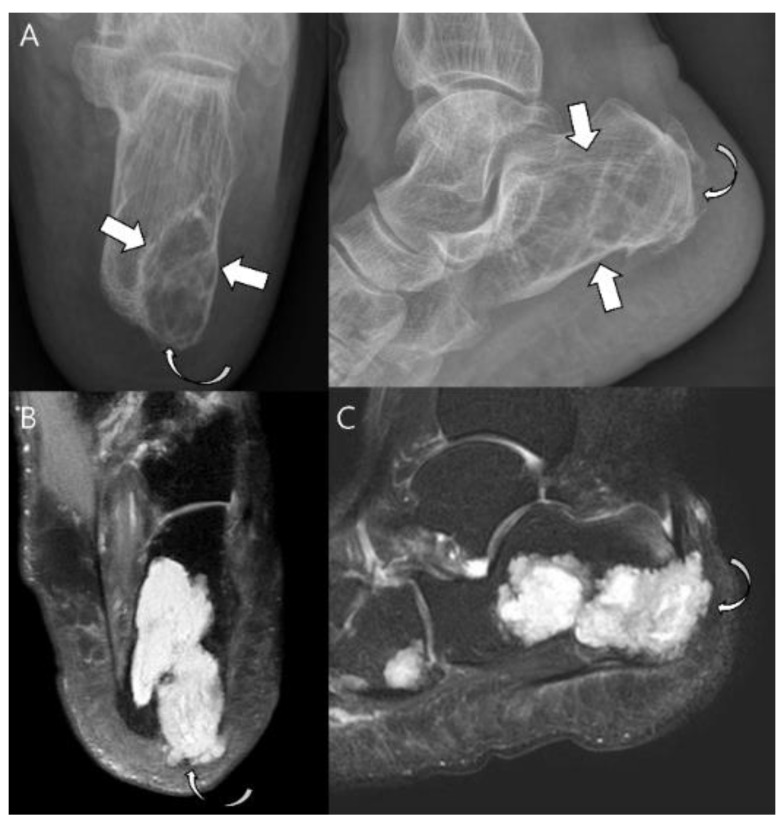
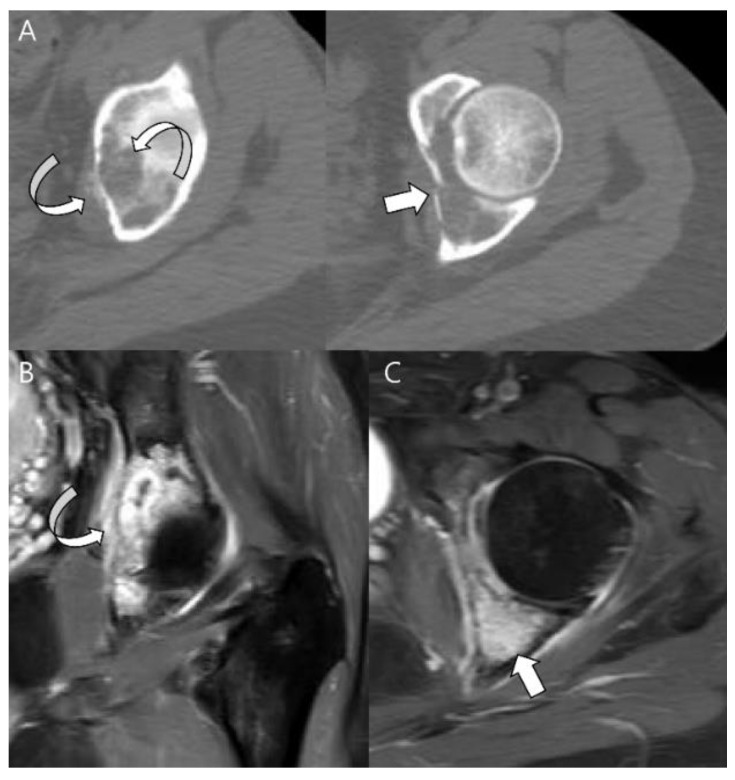
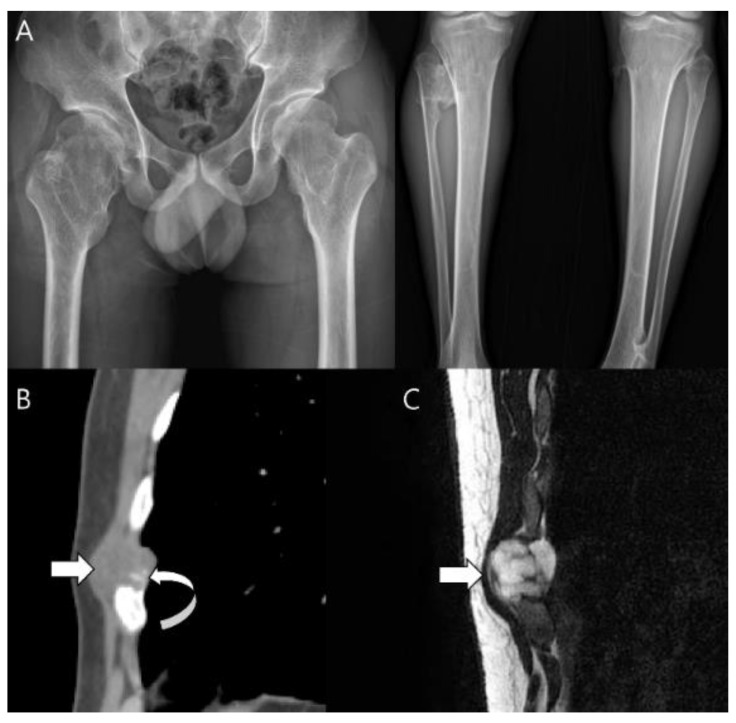
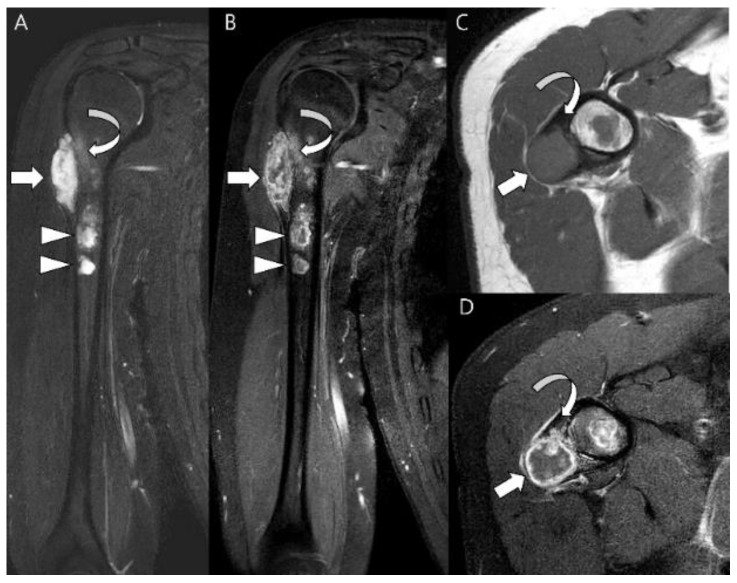
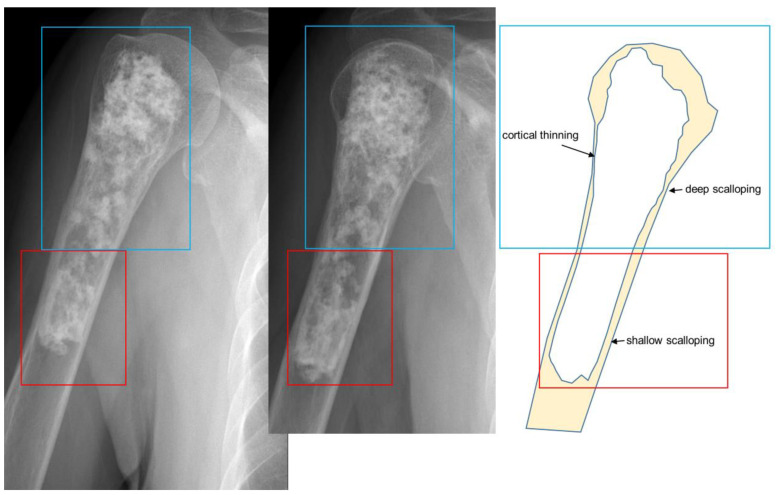
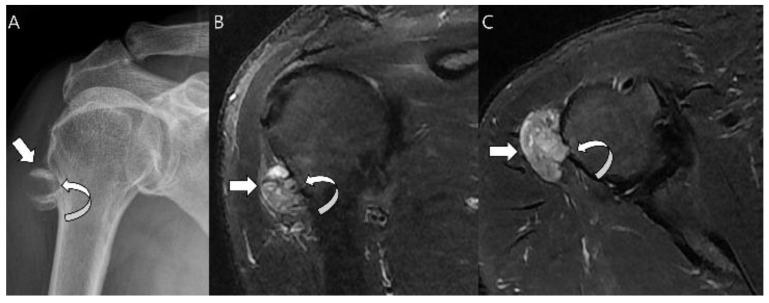
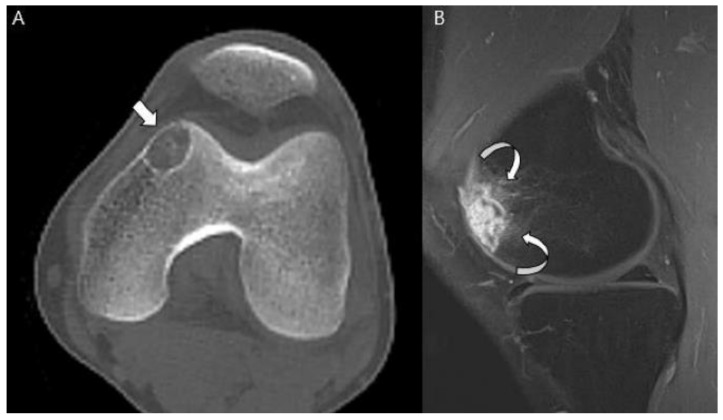
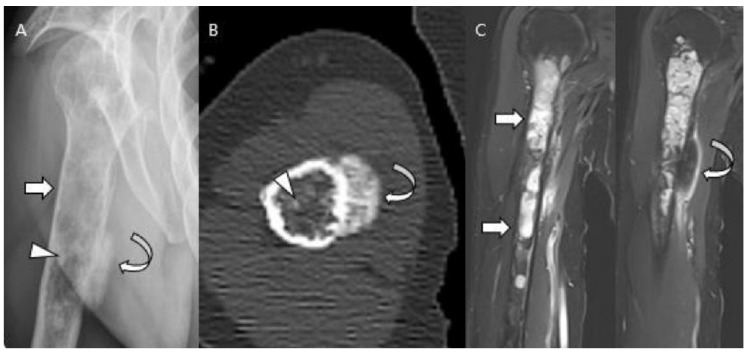
Chondrosarcomas can be classified into various forms according to the presence or absence of a precursor lesion, location, and histological subtype. The new 2020 World Health Organization (WHO) Classification of Tumors of Soft Tissue and Bone classifies chondrogenic bone tumors as benign, intermediate (locally aggressive), or malignant, and separates atypical cartilaginous tumors (ACTs) and chondrosarcoma grade 1 (CS1) as intermediate and malignant tumors. respectively. Furthermore, the classification categorizes chondrosarcomas (including ACT) into eight subtypes: central conventional (grade 1 vs. 2-3), secondary peripheral (grade 1 vs. 2-3), periosteal, dedifferentiated, mesenchymal, and clear cell chondrosarcoma. Most chondrosarcomas are the low-grade, primary central conventional type. The rarer subtypes include clear cell, mesenchymal, and dedifferentiated chondrosarcomas. Comprehensive analysis of the characteristic imaging findings can help differentiate various forms of chondrosarcomas. However, distinguishing low-grade chondrosarcomas from enchondromas or high-grade chondrosarcomas is radiologically and histopathologically challenging, even for experienced radiologists and pathologists.
Keywords: 2020 World Health Organization classification of tumors of soft tissue and bone; atypical cartilaginous tumor; chondrosarcoma; classification; computed tomography; high-grade chondrosarcoma; magnetic resonance imaging; plain radiograph.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
