

Hormone-Related and Drug-Induced Osteoporosis: A Cellular and Molecular Overview
- PMID: 36982891
- PMCID: PMC10054048
- DOI: 10.3390/ijms24065814
Hormone-Related and Drug-Induced Osteoporosis: A Cellular and Molecular Overview
Abstract
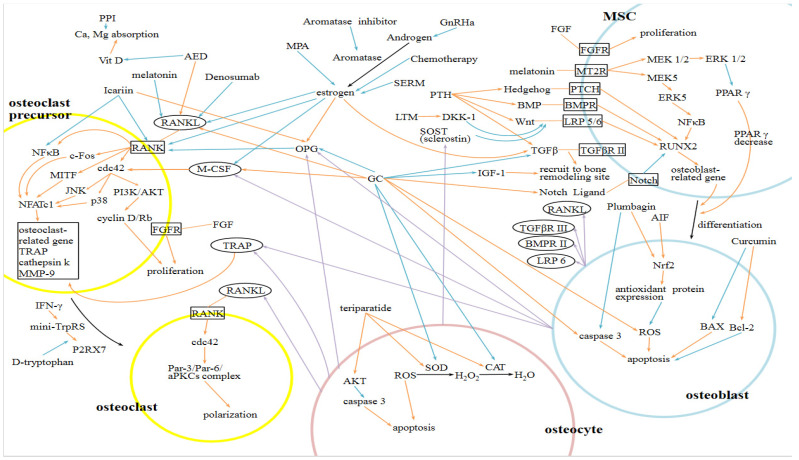
Osteoporosis resulting from an imbalance of bone turnover between resorption and formation is a critical health issue worldwide. Estrogen deficiency following a nature aging process is the leading cause of hormone-related osteoporosis for postmenopausal women, while glucocorticoid-induced osteoporosis remains the most common in drug-induced osteoporosis. Other medications and medical conditions related to secondary osteoporosis include proton pump inhibitors, hypogonadism, selective serotonin receptor inhibitors, chemotherapies, and medroxyprogesterone acetate. This review is a summary of the cellular and molecular mechanisms of bone turnover, the pathophysiology of osteoporosis, and their treatment. Nuclear factor-κβ ligand (RANKL) appears to be the critical uncoupling factor that enhances osteoclastogenesis. In contrast, osteoprotegerin (OPG) is a RANKL antagonist secreted by osteoblast lineage cells. Estrogen promotes apoptosis of osteoclasts and inhibits osteoclastogenesis by stimulating the production of OPG and reducing osteoclast differentiation after suppression of IL-1 and TNF, and subsequent M-CSF, RANKL, and IL-6 release. It can also activate the Wnt signaling pathway to increase osteogenesis, and upregulate BMP signaling to promote mesenchymal stem cell differentiation from pre-osteoblasts to osteoblasts rather than adipocytes. Estrogen deficiency leads to the uncoupling of bone resorption and formation; therefore, resulting in greater bone loss. Excessive glucocorticoids increase PPAR-2 production, upregulate the expression of Dickkopf-1 (DKK1) in osteoblasts, and inhibit the Wnt signaling pathway, thus decreasing osteoblast differentiation. They promote osteoclast survival by enhancing RANKL expression and inhibiting OPG expression. Appropriate estrogen supplement and avoiding excessive glucocorticoid use are deemed the primary treatment for hormone-related and glucocorticoid-induced osteoporosis. Additionally, current pharmacological treatment includes bisphosphonates, teriparatide (PTH), and RANKL inhibitors (such as denosumab). However, many detailed cellular and molecular mechanisms underlying osteoporosis seem complicated and unexplored and warrant further investigation.
Keywords: estrogen; glucocorticoid; hormone; nuclear factor-κβ ligand (RANKL); osteoporosis; osteoprotegerin (OPG).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Chapurlat R., Bui M., Sornay-Rendu E., Zebaze R., Delmas P.D., Liew D., Lespessailles E., Seeman E. Deterioration of Cortical and Trabecular Microstructure Identifies Women With Osteopenia or Normal Bone Mineral Density at Imminent and Long-Term Risk for Fragility Fracture: A Prospective Study. J. Bone Miner. Res. 2019;35:833–844. doi: 10.1002/jbmr.3924. - DOI - PMC - PubMed
-
- Svejme O., Ahlborg H., Nilsson J.-Å., Karlsson M. Early menopause and risk of osteoporosis, fracture and mortality: A 34-year prospective observational study in 390 women: Early menopause and osteoporosis, fracture and mortality. BJOG Int. J. Obstet. Gynaecol. 2012;119:810–816. doi: 10.1111/j.1471-0528.2012.03324.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
