

Pathogenesis, Diagnosis and Management of Squamous Cell Carcinoma and Pseudoepithelial Hyperplasia Secondary to Red Ink Tattoo: A Case Series and Review
- PMID: 36983424
- PMCID: PMC10056737
- DOI: 10.3390/jcm12062424
Pathogenesis, Diagnosis and Management of Squamous Cell Carcinoma and Pseudoepithelial Hyperplasia Secondary to Red Ink Tattoo: A Case Series and Review
Abstract
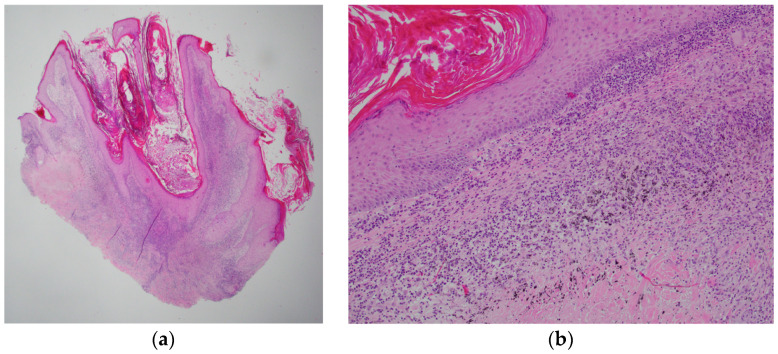
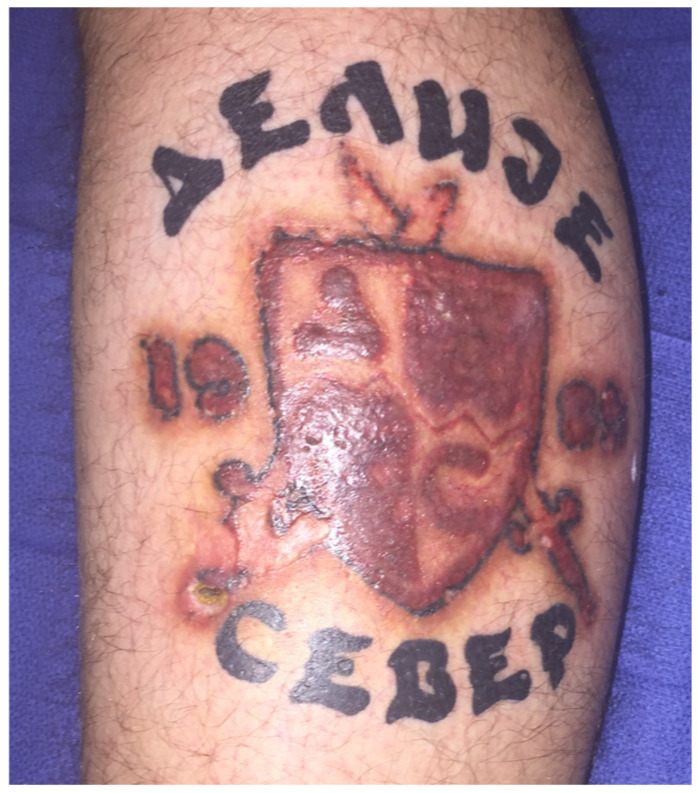
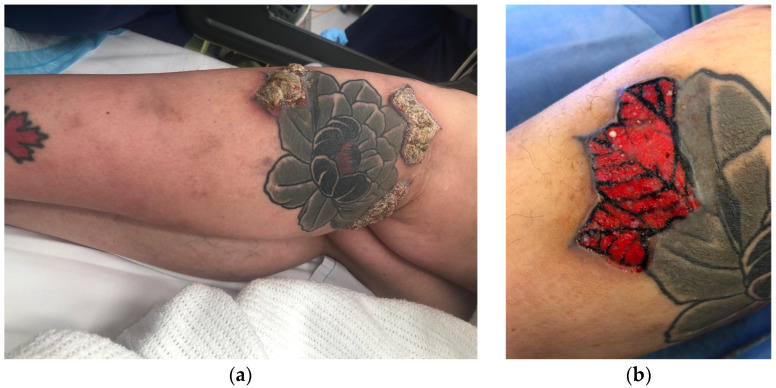
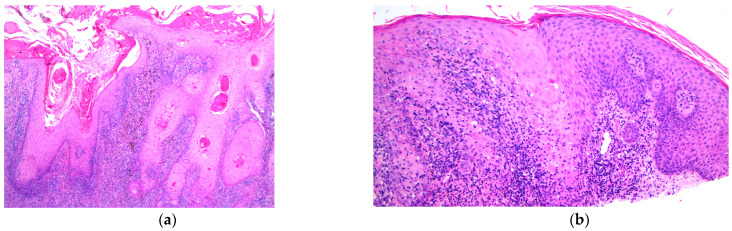
The increasing popularity of tattooing has paralleled an increase in associated cutaneous reactions. Red ink is notorious for eliciting cutaneous reactions. A common reaction is pseudoepitheliomatous hyperplasia (PEH), which is a benign condition closely simulating squamous cell carcinoma (SCC). Differentiating PEH from SCC is challenging for pathologists and clinicians alike. The exact pathogenesis of these lesions secondary to red ink is not known, and there are no sources outlining diagnostic and treatment options and their efficacy. We present four study cases with different pathologies associated to red ink tattoos including lichenoid reaction, granulomatous reaction, PEH, and an SCC. Additionally, an extensive review of 63 articles was performed to investigate pathogenesis, diagnostic approaches, and treatment options. Hypotheses surrounding pathogenesis include but are not limited to the carcinogenic components of pigments, their reaction with UV and the traumatic process of tattooing. Pathogenesis seems to be multifactorial. Full-thickness biopsies with follow-up is the recommended diagnostic approach. There is no evidence of a single universally successful treatment for PEH. Low-dose steroids are usually tried following a step up in lack of clinical response. For SCC lesions, full surgical excision is widely used. A focus on clinicians' awareness of adverse reactions is key for prevention. Regulation of the unmonitored tattoo industry remains an ongoing problem.
Keywords: diagnosis; pseudoepitheliomatous hyperplasia; red; squamous cell carcinoma; tattooing; treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Late-onset pseudoepitheliomatous hyperplasia developing within a red ink tattoo.Dermatol Online J. 2019 May 15;25(5):13030/qt7rk415vm. Dermatol Online J. 2019. PMID: 31220900
-
[Keratoacanthomas on recent tattoos: Two cases].Ann Dermatol Venereol. 2017 Dec;144(12):776-783. doi: 10.1016/j.annder.2017.10.006. Epub 2017 Nov 7. Ann Dermatol Venereol. 2017. PMID: 29126557 French.
-
Complications of decorative tattoos: recognition and management.Am J Clin Dermatol. 2014 Dec;15(6):525-36. doi: 10.1007/s40257-014-0100-x. Am J Clin Dermatol. 2014. PMID: 25385257 Review.
-
A Case of Squamous Cell Carcinoma Developing Within a Red-Ink Tattoo.J Cutan Med Surg. 2017 Jan/Feb;21(1):61-63. doi: 10.1177/1203475416661311. Epub 2016 Sep 22. J Cutan Med Surg. 2017. PMID: 27624899
-
Recurrent lichenoid reaction to black tattoo ink: A case report and brief review of the literature.Australas J Dermatol. 2020 May;61(2):e238-e240. doi: 10.1111/ajd.13231. Epub 2019 Dec 27. Australas J Dermatol. 2020. PMID: 31880811 Review.
Cited by
-
Current and Emerging Insights into the Causes, Immunopathogenesis, and Treatment of Cutaneous Squamous Cell Carcinoma.Cancers (Basel). 2025 May 19;17(10):1702. doi: 10.3390/cancers17101702. Cancers (Basel). 2025. PMID: 40427199 Free PMC article. Review.
-
Pink and Orange Tattoo Pigments: Two Occurrences of Squamous Cell Neoplasms.Cureus. 2024 Apr 25;16(4):e58998. doi: 10.7759/cureus.58998. eCollection 2024 Apr. Cureus. 2024. PMID: 38800316 Free PMC article.
-
A Report of a Keratoacanthoma-Type Cutaneous Squamous Cell Carcinoma Arising Within a Multicolored Ink Tattoo.J Clin Aesthet Dermatol. 2024 Apr;17(4):33-36. J Clin Aesthet Dermatol. 2024. PMID: 38638186 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
