

Duodenal Gangliocytic Paragangliomas-Case Series and Literature Review
- PMID: 36983753
- PMCID: PMC10058500
- DOI: 10.3390/life13030597
Duodenal Gangliocytic Paragangliomas-Case Series and Literature Review
Abstract
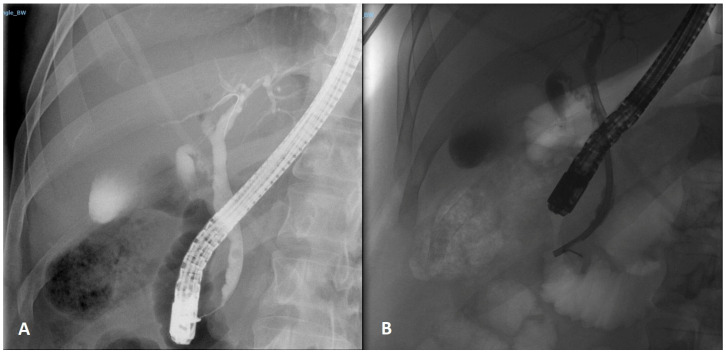
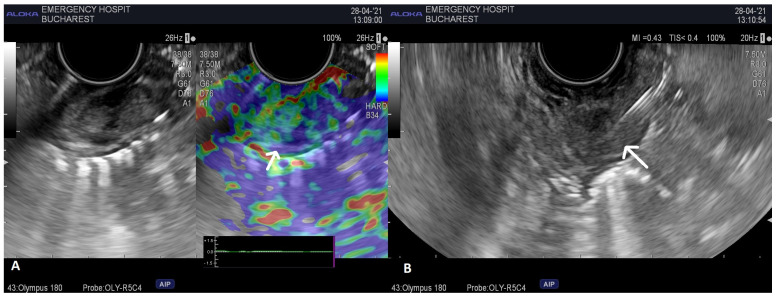
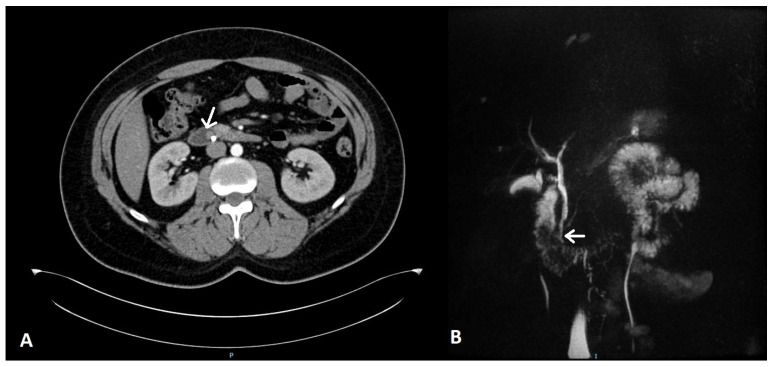
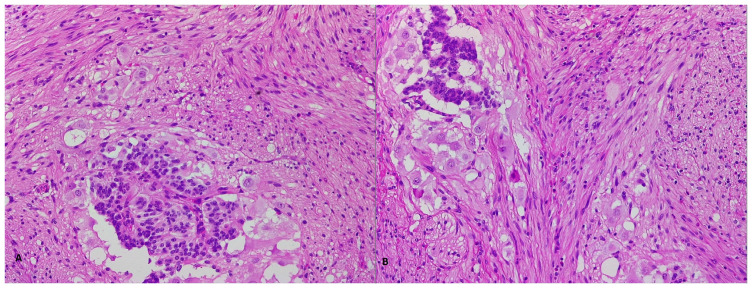
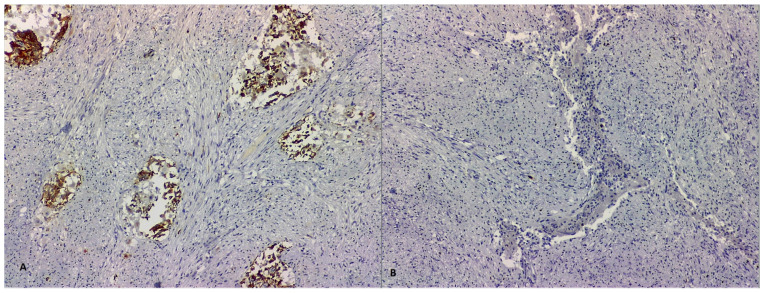
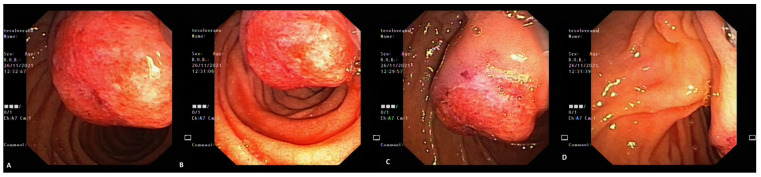
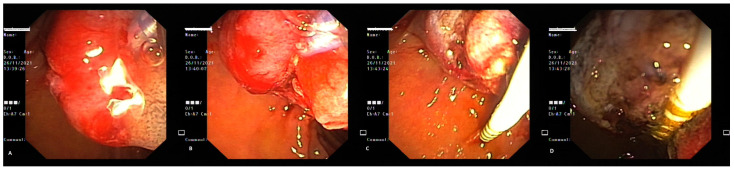
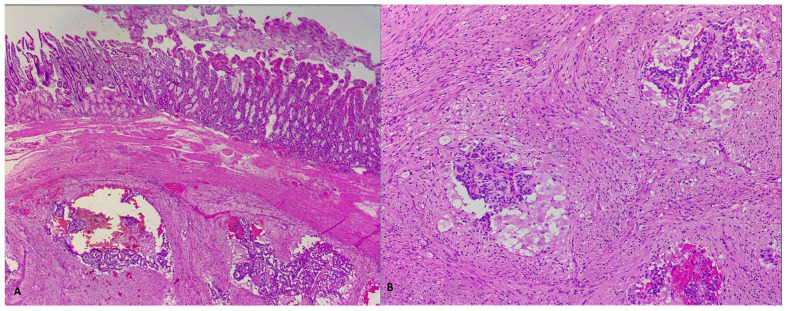
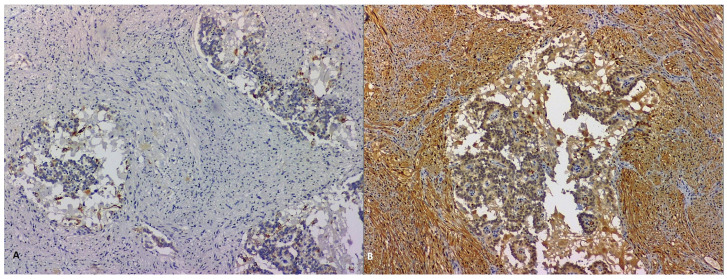
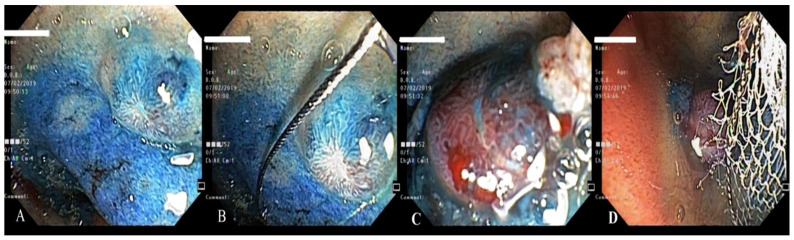
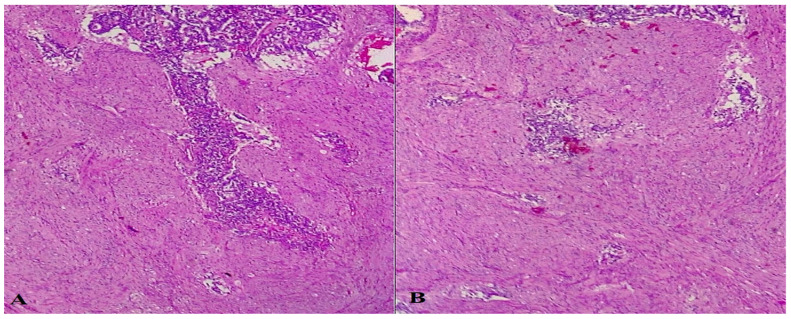
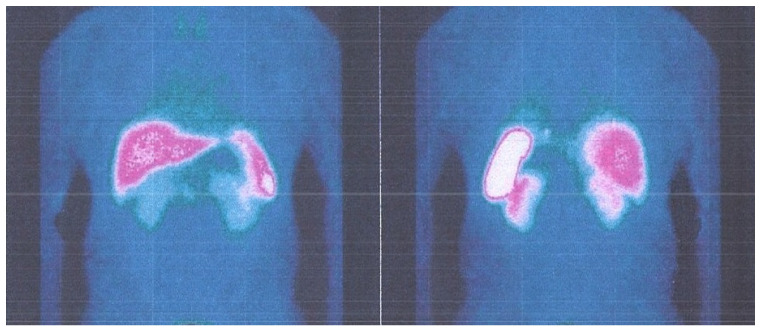
Duodenal gangliocytic paragangliomas are rare neuroendocrine tumors primarily localized in the periampullary area. Though mostly asymptomatic, they can present with various symptoms, most often jaundice, anemia and abdominal pain. The present paper is a case series report, describing our personal experience with patients presenting to the Emergency Unit with different symptoms due to duodenal gangliocytic paraganglioma. Endoscopic resection is safe and indicated in most of the cases, being also associated with lower medical costs. EUS plays a central role in the pre-resection management and in surveillance, and immunostaining is decisive to ascertain the tumor histologic origin. In addition to reporting our experience, we researched the literature regarding these rare tumors and performed a comprehensive review.
Keywords: duodenal gangliocytic paraganglioma; endoscopy; gastrointestinal bleeding; immunohistochemistry; jaundice; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Okubo Y., Yokose T., Motohashi O., Miyagi Y., Yoshioka E., Suzuki M., Washimi K., Kawachi K., Nito M., Nemoto T., et al. Duodenal Rare Neuroendocrine Tumor: Clinicopathological Characteristics of Patients with Gangliocytic Paraganglioma. Gastroenterol. Res. Pract. 2016;2016:5257312. doi: 10.1155/2016/5257312. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
