

Multidisciplinary Therapeutic Management in Complex Cervical Trauma
- PMID: 36984596
- PMCID: PMC10056657
- DOI: 10.3390/medicina59030596
Multidisciplinary Therapeutic Management in Complex Cervical Trauma
Abstract
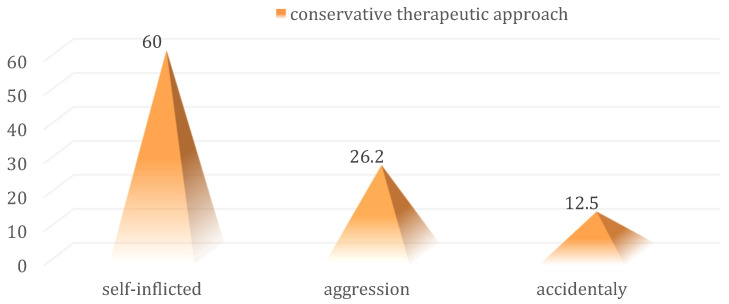
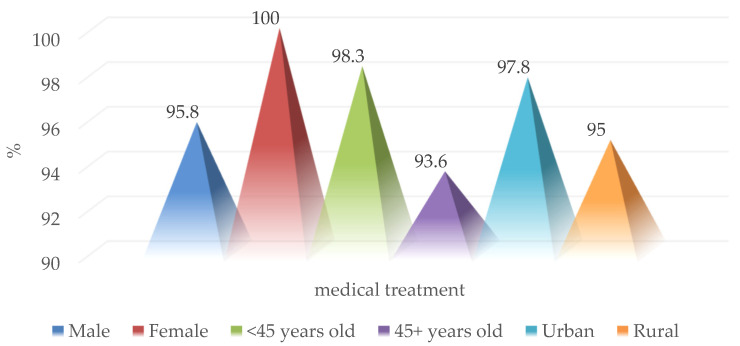
Background and Objectives: In the current literature, mandatory surgical exploration is a controversial topic, with some advocating for it and others against it, proposing a selective conservative management. This multidisciplinary therapeutic approach is based on clinical examination and serial paraclinical explorations associated with supportive drug treatment. Materials and Methods: The study group consisted of 103 patients with complex cervical trauma pathology produced by various mechanisms such as car or domestic accidents, aggression, ballistic trauma, self-inflicted attempts, hanging or strangulation hospitalized in the Ear, Nose and Throat (E.N.T.) Clinic, at "St. Spiridon" Iași Hospital, between 2012 and 2016. Results: The universal clinical indication for urgent surgical exploration of the patient with complex cervical trauma is the presence of the following symptoms: unstable vital signs, significant pulsatile bleeding, hematoma with a substantial increase in size, shock, airway obstruction, open airway wound, hematemesis, or hemoptysis. In this context, we considered it worthwhile to research the management of complex cervical trauma in a reference university medical center, alongside the analysis of the patient's characteristics under different aspects (demographic, pathological aspects, therapeutic). Conclusions: Complex cervical trauma has a variety of clinical aspects, with a variable evolution, which involves multidisciplinary therapeutic management. The increasing trauma rate is one of the main public health problems, requiring epidemiological studies, and the implementation of control strategies.
Keywords: complex cervical trauma; multidisciplinary treatment; otorhinolaryngology; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
