

The Role of Biomarkers and Scores in Describing Urosepsis
- PMID: 36984597
- PMCID: PMC10059648
- DOI: 10.3390/medicina59030597
The Role of Biomarkers and Scores in Describing Urosepsis
Abstract
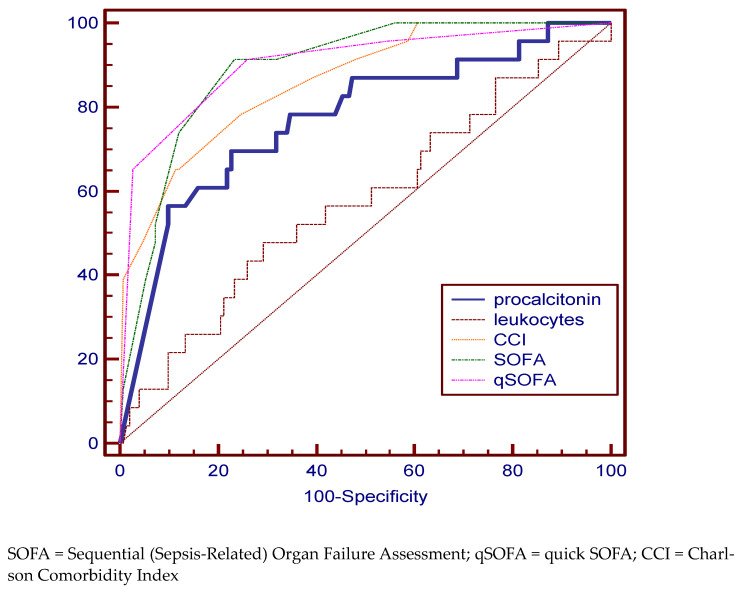
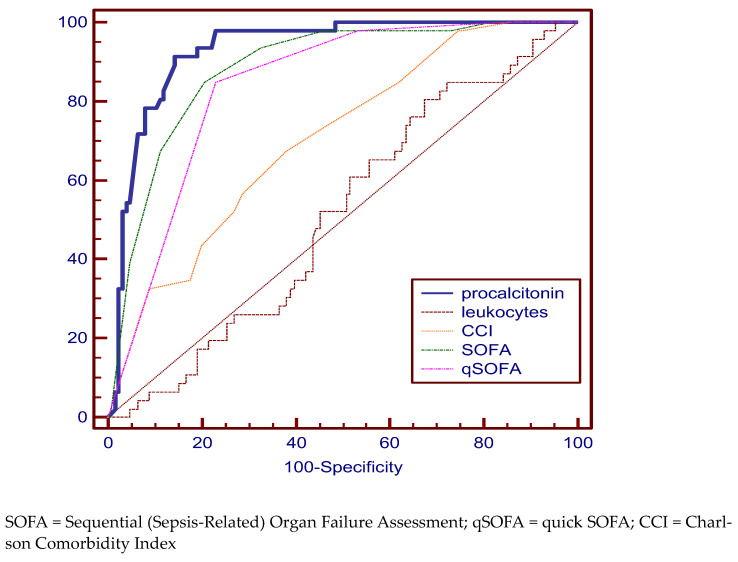
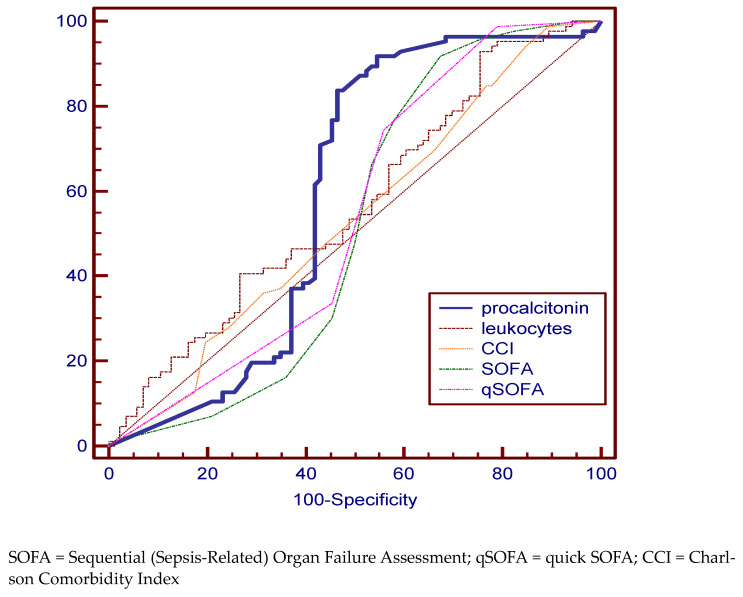
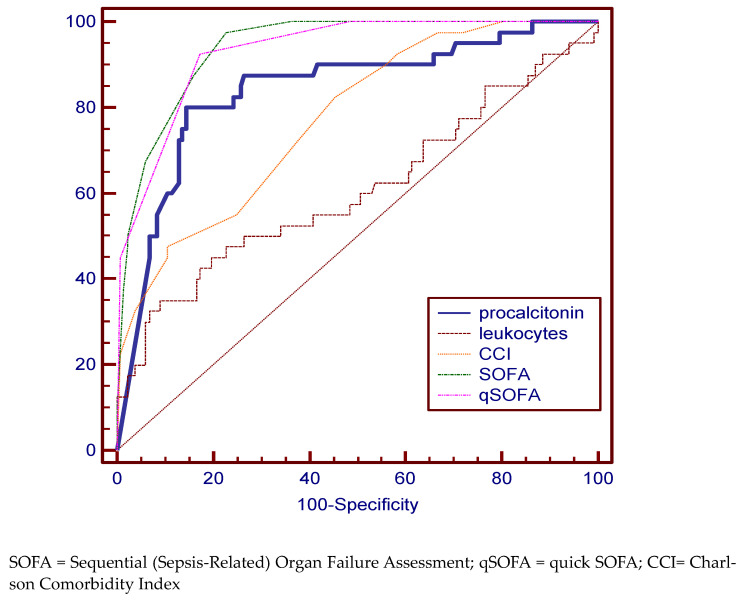
Background and Objectives: Patients with urinary tract obstruction (UTO) and systemic inflammatory response syndrome (SIRS) are at risk of developing urosepsis, whose evolution involves increased morbidity, mortality and cost. The aim of this study is to evaluate the ability of already existing scores and biomarkers to diagnose, describe the clinical status, and predict the evolution of patients with complicated urinary tract infection (UTI) and their risk of progressing to urosepsis. Materials and Methods: We conducted a retrospective study including patients diagnosed with UTI hospitalized in the urology department of" Sfântul Apostol Andrei" County Emergency Clinical Hospital (GCH) in Galati, Romania, from September 2019 to May 2022. The inclusion criteria were: UTI proven by urine culture or diagnosed clinically complicated with UTO, fever or shaking chills, and purulent collections, such as psoas abscess, Fournier Syndrome, renal abscess, and paraurethral abscess, showing SIRS. The exclusion criteria were: patients age < 18 years, pregnancy, history of kidney transplantation, hemodialysis or peritoneal dialysis, and patients with missing data. We used the Sequential (Sepsis-Related) Organ Failure Assessment (SOFA) and qSOFA (quick SOFA) scores, and procalcitonin (PCT) to describe the clinical status of the patients. The Charlson Comorbidity Index (CCI) was used to assesses pre-existing morbidities. The hospitalization days and costs and the days of intensive care were considered. Depending on the diagnosis at admission, we divided the patients into three groups: SIRS, sepsis and septic shock. The fourth group was represented by patients who died during hospitalization. Results: A total of 174 patients with complicated UTIs were enrolled in this study. From this total, 46 were enrolled in the SIRS group, 88 in the urosepsis group, and 40 in the septic shock group. A total of 23 patients died during hospitalization and were enrolled in the deceased group. An upward trend of age along with worsening symptoms was highlighted with an average of 56.86 years in the case of SIRS, 60.37 years in the sepsis group, 69.03 years in the septic shock, and 71.04 years in the case of deceased patients (p < 0.04). A statistically significant association between PCT and complex scores (SOFA, CCI and qSOFA) with the evolution of urosepsis was highlighted. Increased hospitalization costs can be observed in the case of deceased patients and those with septic shock and statistically significantly lower in the case of those with SIRS. The predictability of discriminating urosepsis stages was assessed by using the area under the ROC curve (AUC) and very good specificity and sensitivity was identified in predicting the risk of death for PCT (69.57%, 77.33%), the SOFA (91.33%, 76.82%), qSOFA (91.30%, 74.17%) scores, and CCI (65.22%, 88.74%). The AUC value was best for qSOFA (90.3%). For the SIRS group, the PCT (specificity 91.30%, sensitivity 85.71%) and SOFA (specificity 84.78%, sensitivity 78.74%), qSOFA scores (specificity 84.78%, sensitivity 76, 34%) proved to be relevant in establishing the diagnosis. In the case of the septic shock group, the qSOFA (specificity 92.5%, sensitivity 82.71%) and SOFA (specificity 97.5%, sensitivity 77.44%) as well as PCT (specificity 80%, sensitivity 85.61%) are statistically significant disease-defining variables. An important deficit in the tools needed to classify patients into the sepsis group is obvious. All the variables have an increased specificity but a low sensitivity. This translates into a risk of a false negative diagnosis. Conclusions: Although SOFA and qSOFA scores adequately describe patients with septic shock and they are independent prognostic predictors of mortality, they fail to be accurate in diagnosing sepsis. These scores should not replace the conventional triage protocol. In our study, PCT proved to be a disease-defining marker and an independent prognostic predictor of mortality. Patients with important comorbidities, CCI greater than 10, should be treated more aggressively because of increased mortality.
Keywords: biomarkers; diagnosis; sensitivity and specificity; sepsis; urinary tract infection.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Naber K.G., Bergman B., Bishop M.C., Bjerklund-Johansen T.E., Botto H., Lobel B., Jinenez Cruz F., Selvaggi F.P. Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU) EAU guidelines for the management of urinary and male genital tract infections. Urinary Tract Infection (UTI) Working Group of the Health Care Office (HCO) of the European Association of Urology (EAU). EAU Guidelines for the Management of Urinary and Male Genital Tract Infections. Eur. Urol. 2001;40:576–588. doi: 10.1159/000049840. - DOI - PubMed
-
- Singer M., Deutschman C.S., Seymour C.W., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.-D., Coopersmith C.M., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Levy M.M., Artigas A., Phillips G.S., Rhodes A., Beale R., Osborn T., Vincent J.-L., Townsend S., Lemeshow S., Dellinger R.P. Outcomes of the Surviving Sepsis Campaign in intensive care units in the USA and Europe: A prospective cohort study. Lancet Infect. Dis. 2012;12:919–924. doi: 10.1016/S1473-3099(12)70239-6. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
