

Long-term Quality of Life and Functional Outcome of Patients With Rectal Cancer Following a Watch-and-Wait Approach
- PMID: 36988922
- PMCID: PMC10061319
- DOI: 10.1001/jamasurg.2023.0146
Long-term Quality of Life and Functional Outcome of Patients With Rectal Cancer Following a Watch-and-Wait Approach
Abstract
Importance: A watch-and-wait approach for patients with rectal cancer and a clinical complete response after neoadjuvant chemoradiotherapy or radiotherapy is associated with better quality of life and functional outcome. Nevertheless, prospective data on both parameters are scarce.
Objective: To prospectively evaluate quality of life and functional outcome, including bowel, urinary, and sexual function, of patients following a watch-and-wait approach.
Design, setting, and participants: A total of 278 patients with rectal cancer and a clinical complete response or near-complete response after neoadjuvant chemoradiotherapy or radiotherapy were included in 2 prospective cohort studies: a single-center study (March 2014 to October 2017) and an ongoing multicenter study (from September 2017). Patients were observed by a watch-and-wait approach. Additional local excision or total mesorectal excision was performed for residual disease or regrowth. Data were analyzed between April 1, 2021, and August 27, 2021, for patients with a minimum follow-up of 24 months.
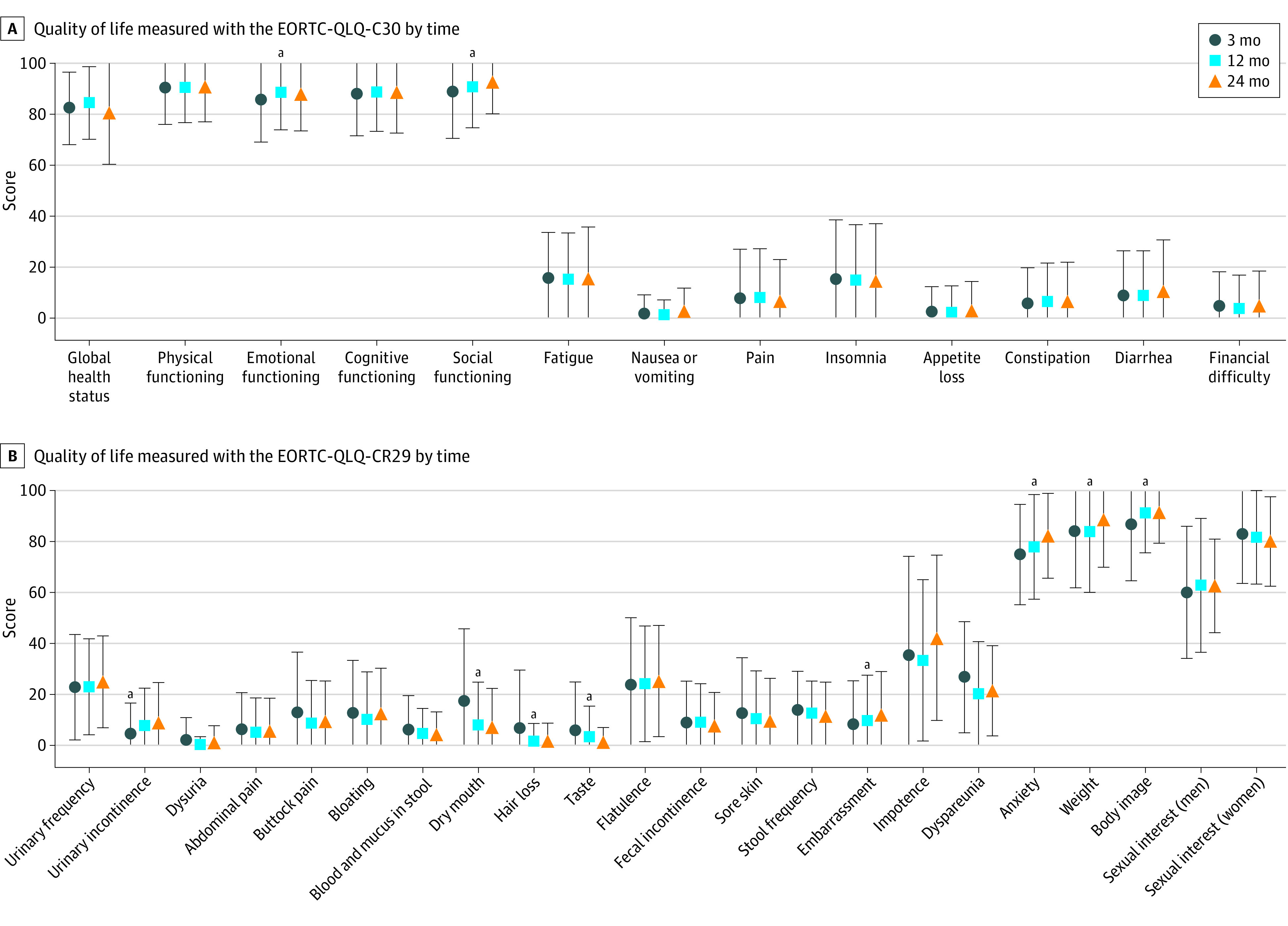
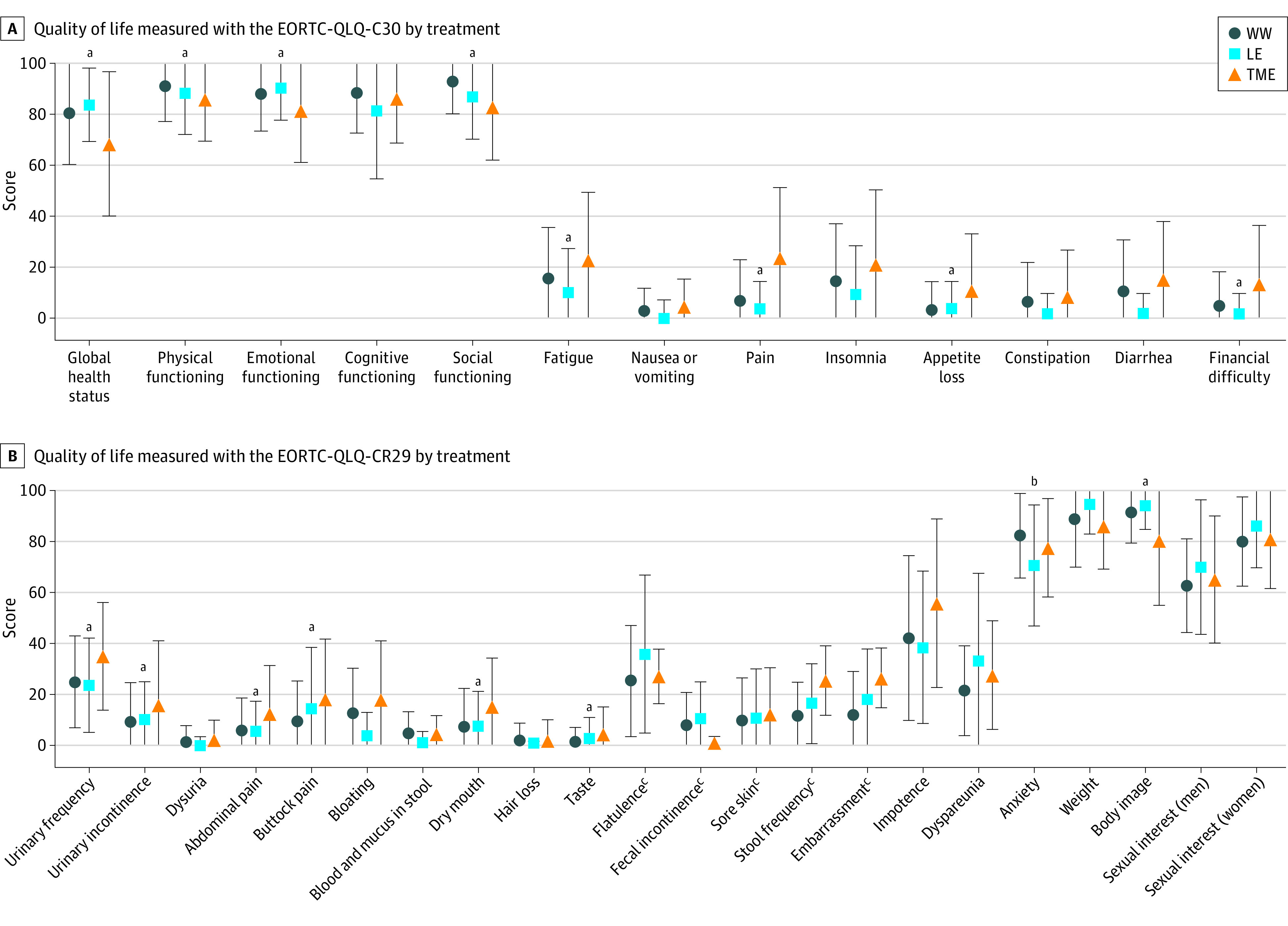
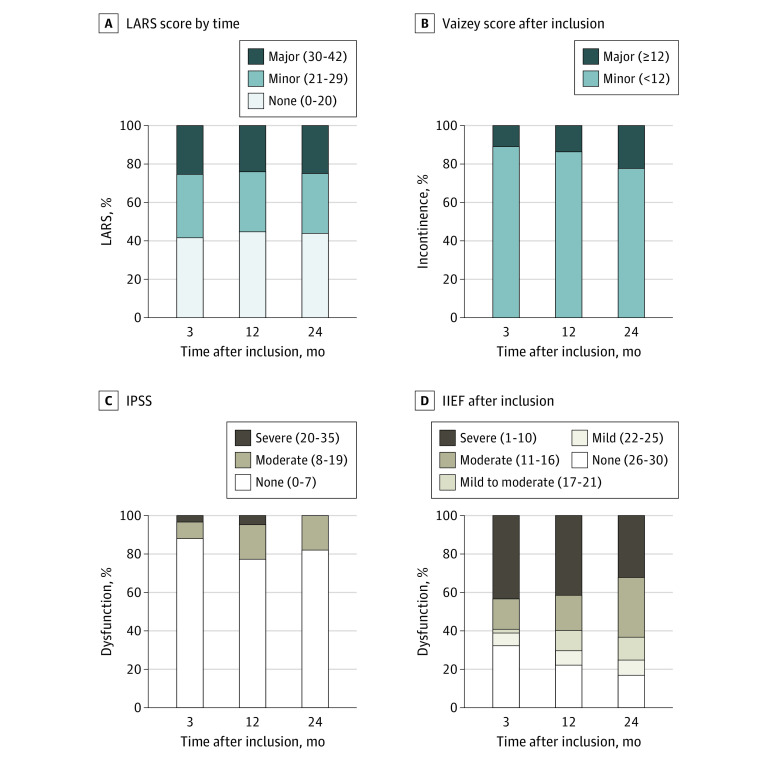
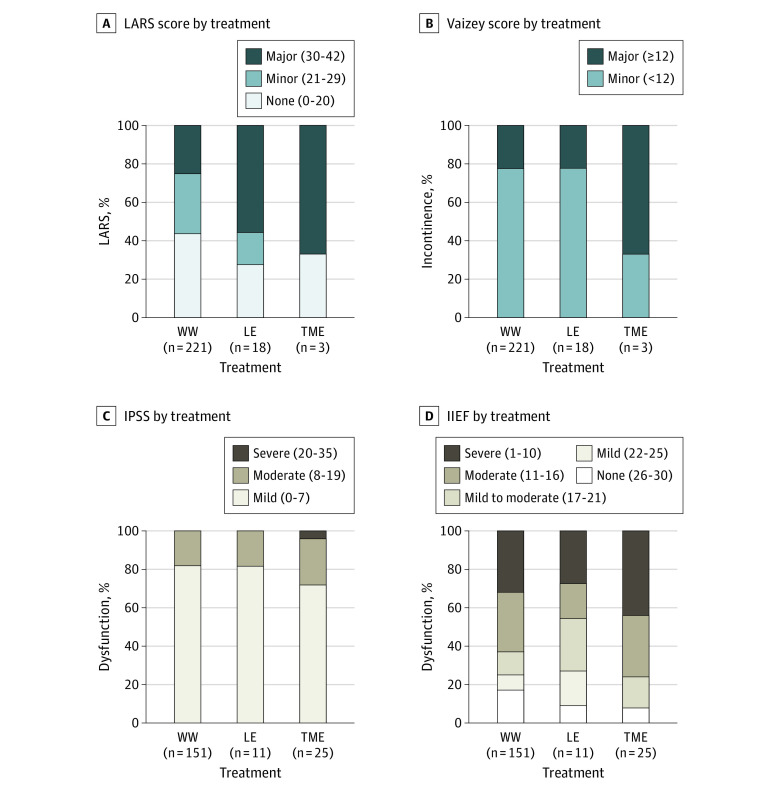
Main outcomes and measures: Quality of life was evaluated with the European Organisation for Research and Treatment of Cancer-Quality of Life Questionnaire-C30 (EORTC-QLQ-C30), EORTC-QLQ-CR38, or EORTC-QLQ-CR29 and 36-Item Short-Form Health Survey. The score for the questionnaires and 36-Item Short-Form Health Survey ranges from 0 to 100. For some scales, a high score indicates a high level of functioning, and for others it indicates a high level of complaints and symptomatology. Functional outcome was assessed by the Low Anterior Resection Syndrome score, Vaizey incontinence score, International Prostate Symptom Score, International Index of Erectile Function, and Female Sexual Function Index.
Results: Of 278 patients included, 187 were male (67%), and the median age was 66 years (range, 34-85 years). In the first 24 months, 221 patients (80%) were observed by a watch-and-wait approach without requiring surgery, 18 patients (6%) underwent additional local excision, and 39 patients (14%) underwent total mesorectal excision. In general, patients observed by a watch-and-wait approach reported good quality of life, with limited variation over time. At 3 months, 56 of 221 patients (25.3%) reported major bowel dysfunction; at 12 months, 53 patients (24.0%) reported it; and at 24 months, 55 patients (24.9%) reported it. At 24 months, 48 of 151 male patients (31.8%) reported severe erectile dysfunction. For female patients, sexual satisfaction and overall sexual function decreased during follow-up. Patients who underwent local excision reported more major bowel dysfunction (10 of 18 patients [55.6%]) compared with those without additional surgery. Quality-of-life scores, however, were comparable. After total mesorectal excision, patients scored significantly worse on several quality-of-life subscales.
Conclusions and relevance: Results of this study suggest that patients with rectal cancer who were observed by a watch-and-wait approach had good quality of life, with some patients reporting bowel and sexual dysfunction. Quality of life and functional outcome deteriorated when patients required surgery. These data will be useful in daily care to counsel patients on what to expect from a watch-and-wait approach.
Conflict of interest statement
Figures
Comment in
-
Guiding Patients Through a "Watch-and-Wait" Approach for Rectal Cancer-Understanding the Functional Outcomes.JAMA Surg. 2023 May 1;158(5):e230165. doi: 10.1001/jamasurg.2023.0165. Epub 2023 May 10. JAMA Surg. 2023. PMID: 36988979 No abstract available.
References
-
- van der Valk MJM, Hilling DE, Bastiaannet E, et al. ; IWWD Consortium . Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet. 2018;391(10139):2537-2545. doi:10.1016/S0140-6736(18)31078-X - DOI - PubMed
-
- Dossa F, Chesney TR, Acuna SA, Baxter NN. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2017;2(7):501-513. doi:10.1016/S2468-1253(17)30074-2 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
