

Effect of Multimodal Prehabilitation on Reducing Postoperative Complications and Enhancing Functional Capacity Following Colorectal Cancer Surgery: The PREHAB Randomized Clinical Trial
- PMID: 36988937
- PMCID: PMC10061316
- DOI: 10.1001/jamasurg.2023.0198
Effect of Multimodal Prehabilitation on Reducing Postoperative Complications and Enhancing Functional Capacity Following Colorectal Cancer Surgery: The PREHAB Randomized Clinical Trial
Erratum in
-
Errors in Figure 3.JAMA Surg. 2023 Jun 1;158(6):675. doi: 10.1001/jamasurg.2023.1553. JAMA Surg. 2023. PMID: 37133848 Free PMC article. No abstract available.
Abstract
Importance: Colorectal surgery is associated with substantial morbidity rates and a lowered functional capacity. Optimization of the patient's condition in the weeks prior to surgery may attenuate these unfavorable sequelae.
Objective: To determine whether multimodal prehabilitation before colorectal cancer surgery can reduce postoperative complications and enhance functional recovery.
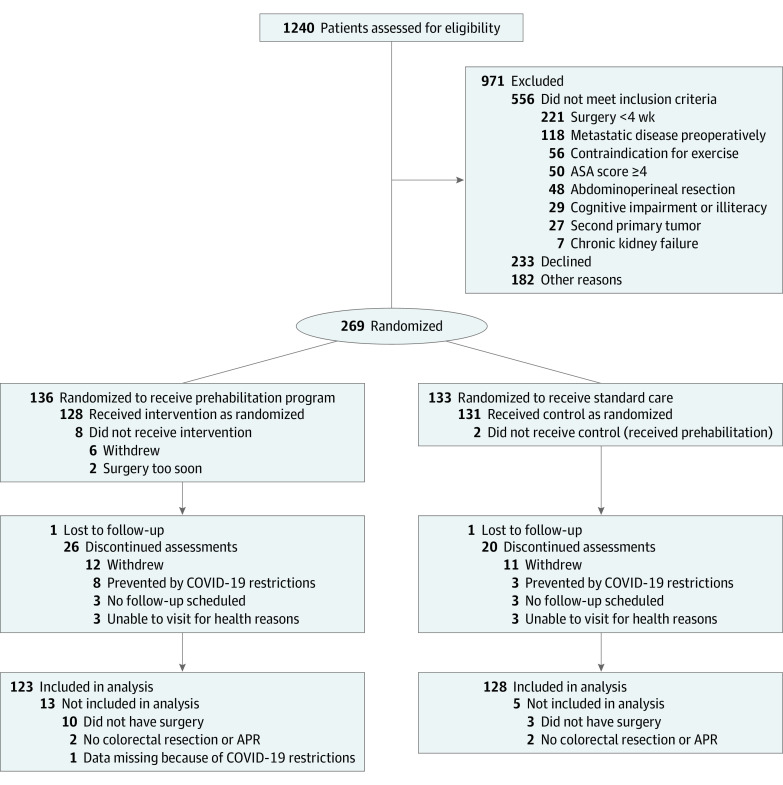
Design, setting, and participants: The PREHAB randomized clinical trial was an international, multicenter trial conducted in teaching hospitals with implemented enhanced recovery after surgery programs. Adult patients with nonmetastasized colorectal cancer were assessed for eligibility and randomized to either prehabilitation or standard care. Both arms received standard perioperative care. Patients were enrolled from June 2017 to December 2020, and follow-up was completed in December 2021. However, this trial was prematurely stopped due to the COVID-19 pandemic.
Interventions: The 4-week in-hospital supervised multimodal prehabilitation program consisted of a high-intensity exercise program 3 times per week, a nutritional intervention, psychological support, and a smoking cessation program when needed.
Main outcomes and measures: Comprehensive Complication Index (CCI) score, number of patients with CCI score more than 20, and improved walking capacity expressed as the 6-minute walking distance 4 weeks postoperatively.
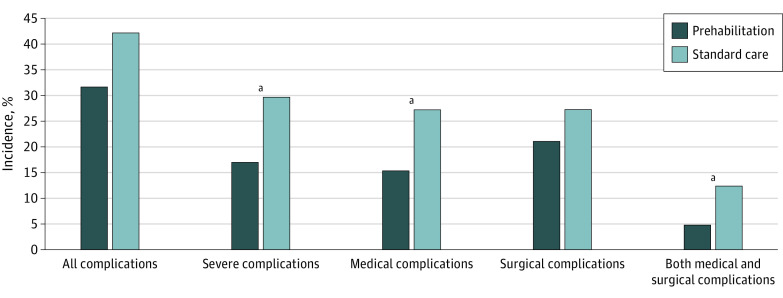
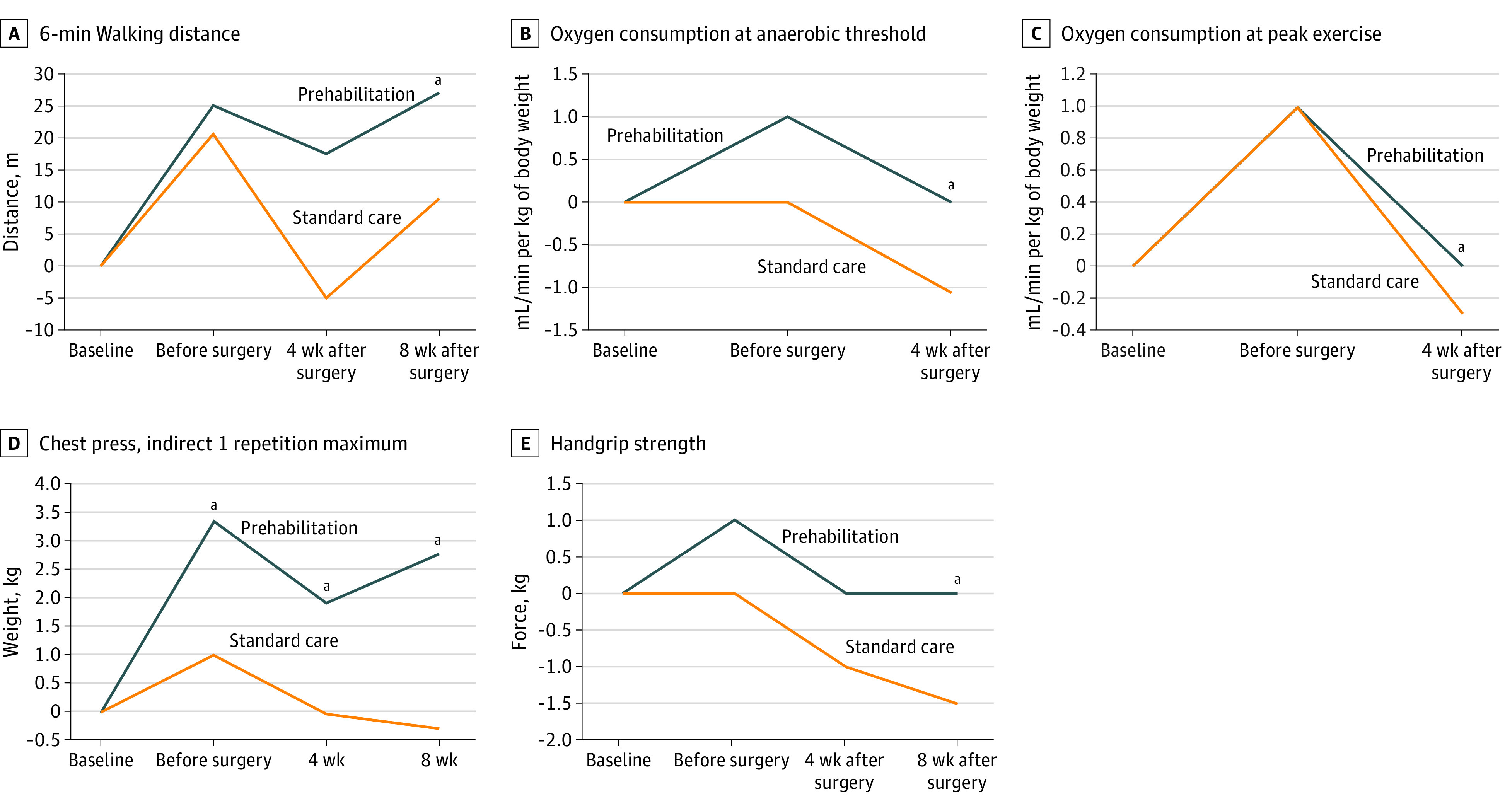
Results: In the intention-to-treat population of 251 participants (median [IQR] age, 69 [60-76] years; 138 [55%] male), 206 (82%) had tumors located in the colon and 234 (93%) underwent laparoscopic- or robotic-assisted surgery. The number of severe complications (CCI score >20) was significantly lower favoring prehabilitation compared with standard care (21 of 123 [17.1%] vs 38 of 128 [29.7%]; odds ratio, 0.47 [95% CI, 0.26-0.87]; P = .02). Participants in prehabilitation encountered fewer medical complications (eg, respiratory) compared with participants receiving standard care (19 of 123 [15.4%] vs 35 of 128 [27.3%]; odds ratio, 0.48 [95% CI, 0.26-0.89]; P = .02). Four weeks after surgery, 6-minute walking distance did not differ significantly between groups when compared with baseline (mean difference prehabilitation vs standard care 15.6 m [95% CI, -1.4 to 32.6]; P = .07). Secondary parameters of functional capacity in the postoperative period generally favored prehabilitation compared with standard care.
Conclusions and relevance: This PREHAB trial demonstrates the benefit of a multimodal prehabilitation program before colorectal cancer surgery as reflected by fewer severe and medical complications postoperatively and an optimized postoperative recovery compared with standard care.
Trial registration: trialregister.nl Identifier: NTR5947.
Conflict of interest statement
Figures
Comment in
-
Overcoming Implementation Challenges With Innovation and Patient Empowerment-Let's Keep Moving With Prehabilitation.JAMA Surg. 2023 Jun 1;158(6):582. doi: 10.1001/jamasurg.2023.0228. JAMA Surg. 2023. PMID: 36988938 No abstract available.
-
Limitations of the PREHAB Randomized Clinical Trial.JAMA Surg. 2023 Dec 1;158(12):1354-1355. doi: 10.1001/jamasurg.2023.3752. JAMA Surg. 2023. PMID: 37647049 No abstract available.
-
Limitations of the PREHAB Randomized Clinical Trial.JAMA Surg. 2023 Dec 1;158(12):1355. doi: 10.1001/jamasurg.2023.3755. JAMA Surg. 2023. PMID: 37647061 No abstract available.
