

Large Left Ventricular Pseudoaneurysm Presenting as an Embolic Stroke After a "Silent" Myocardial Infarction
- PMID: 36988947
- PMCID: PMC10178654
- DOI: 10.14503/THIJ-22-7922
Large Left Ventricular Pseudoaneurysm Presenting as an Embolic Stroke After a "Silent" Myocardial Infarction
Abstract
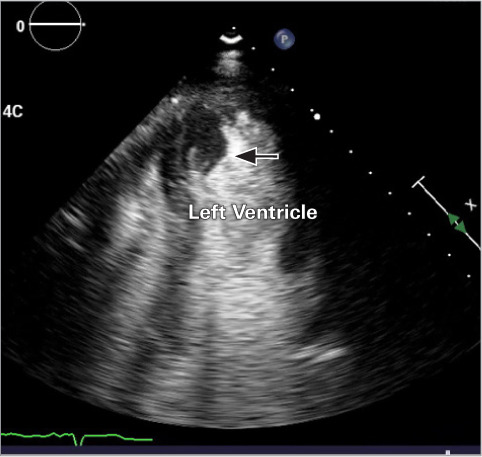
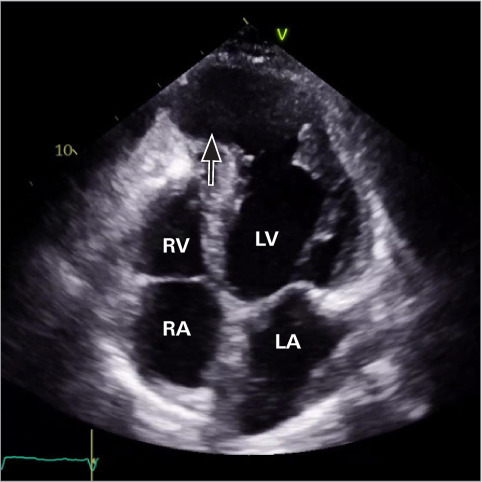
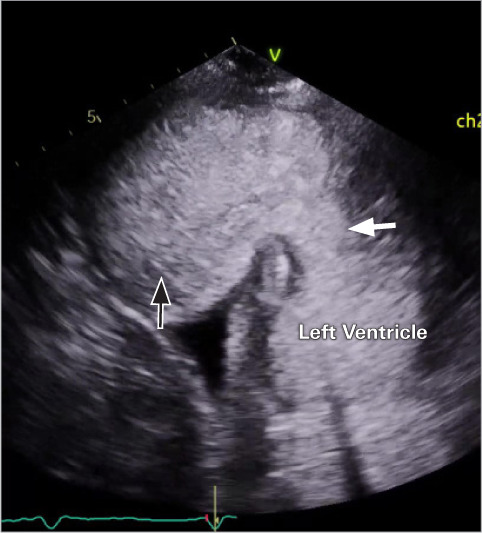
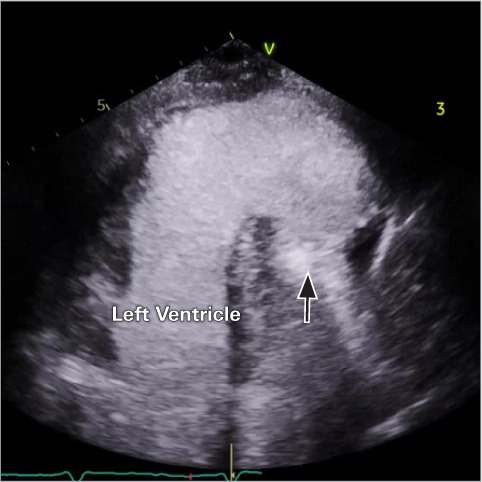
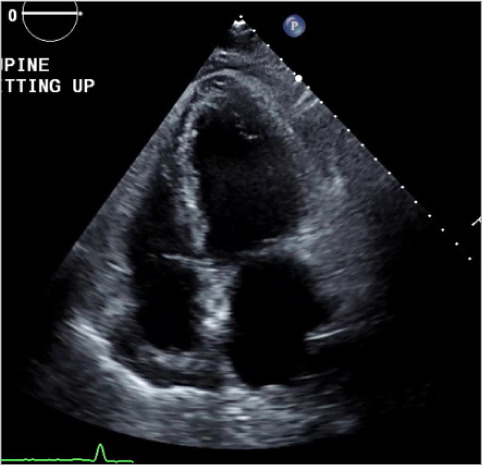
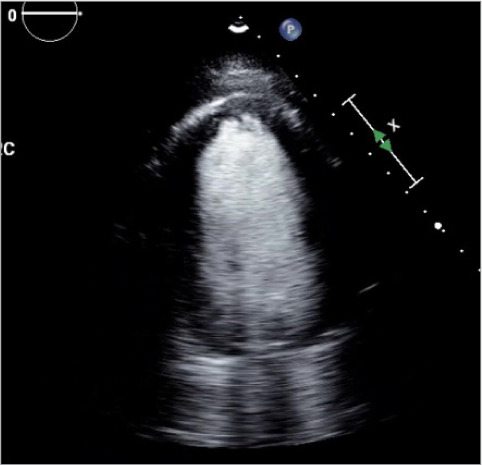
A 72-year-old woman with no history of coronary artery disease presented with an acute left middle cerebral artery stroke and was found to have a large left ventricular pseudoaneurysm measuring 8.7 × 7.6 cm and 2 large left ventricular thrombi, the source of her systemic embolization. Despite initial medical management, she developed refractory New York Heart Association functional class III heart failure, uncontrolled atrial fibrillation, and further enlargement of her pseudoaneurysm to 5.5 × 10.6 × 9.2 cm. She underwent urgent aneurysmectomy. Left ventricular pseudoaneurysms are rare and most commonly occur following an acute myocardial infarction when a ventricular free-wall rupture is contained by pericardium or thrombi. Historically, left ventricular angiography displaying a lack of an overlying coronary artery was the gold standard for diagnosis. Now, noninvasive imaging such as computed tomography, magnetic resonance imaging, and echocardiogram with ultrasound-enhancing agent, are reliable diagnostic tools. They can distinguish a pseudoaneurysm from a true left ventricular aneurysm using characteristic findings such as a narrow aneurysm neck, bidirectional doppler flow between the pseudoaneurysm and the left ventricle, and abrupt changes in the cardiac wall structures. Progressive dilation, wall thinning, and dyskinesis can result in refractory heart failure, arrhythmias, and thrombi formation from venous stasis. Pseudoaneurysms have a 30% to 45% risk of rupture and can be treated with left ventricular aneurysmectomy.
Keywords: Pseudoaneurysm; embolic stroke; myocardial infarction.
© 2023 by the Texas Heart® Institute, Houston.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
