

Association of Glucose-6-Phosphate Dehydrogenase Deficiency With Outcomes in US Veterans With COVID-19
- PMID: 36988953
- PMCID: PMC10061239
- DOI: 10.1001/jamanetworkopen.2023.5626
Association of Glucose-6-Phosphate Dehydrogenase Deficiency With Outcomes in US Veterans With COVID-19
Abstract
Importance: The underlying biological risk factors for severe outcome due to SAR-CoV-2 infection are not well defined.
Objective: To determine the association between glucose-6-phosphate dehydrogenase (G6PD) deficiency and severity of COVID-19.
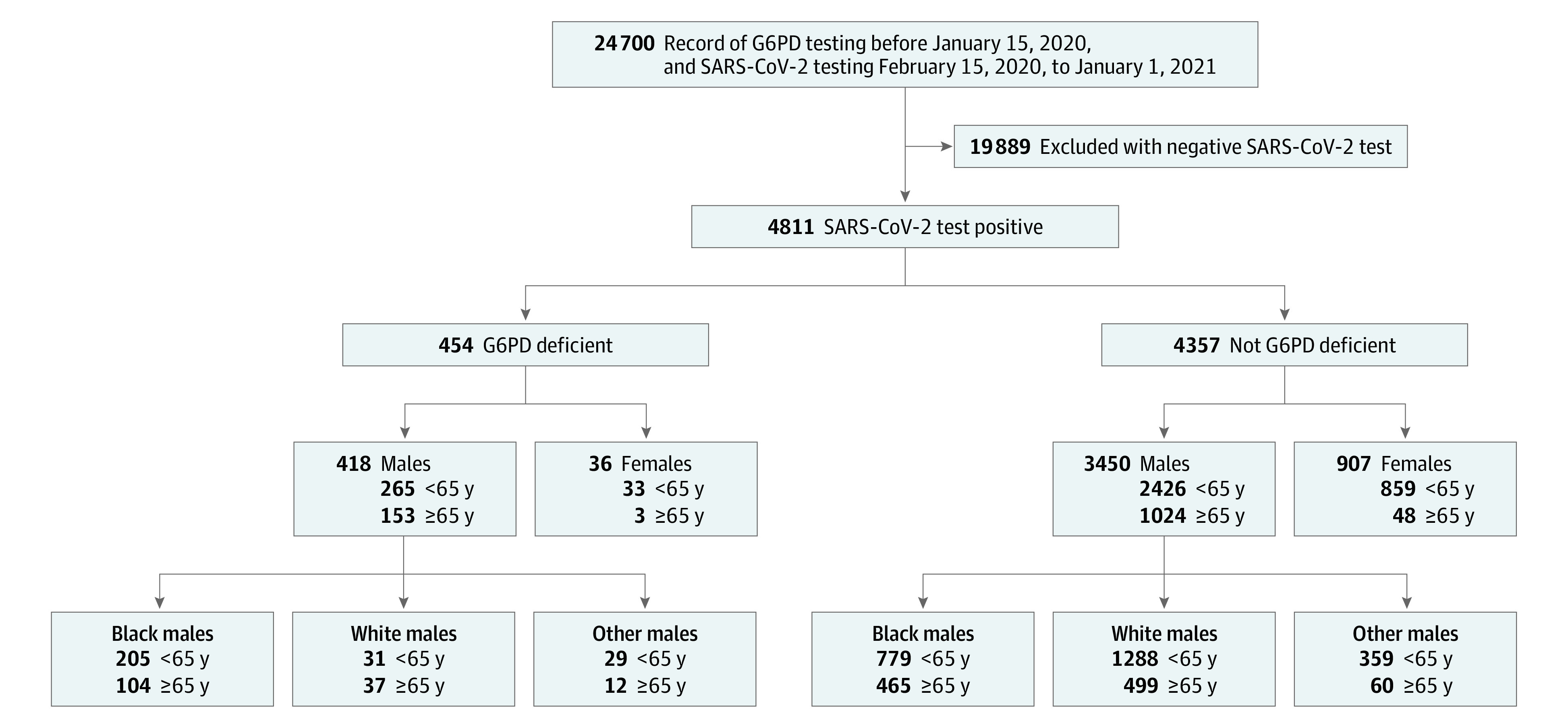
Design, setting, and participants: This retrospective cohort study included analysis of 24 700 veterans with G6PD enzyme testing prior to January 1, 2020, obtained through the US Veterans Health Administration national databases. These veterans were cross-referenced with the Veterans Administration COVID-19 Shared Data Resource for SARS-CoV-2 testing from February 15, 2020, to January 1, 2021. The final study population consisted of 4811 veterans who tested positive for SARS-CoV-2. Statistical analysis was performed from June to December 2021.
Exposures: G6PD deficiency.
Main outcomes and measures: COVID-19 severe illness, as defined by the Centers for Disease Control and Prevention: hospitalization, need for mechanical ventilation and/or intensive care unit admission, or in-hospital mortality after a positive SARS-CoV-2 test.
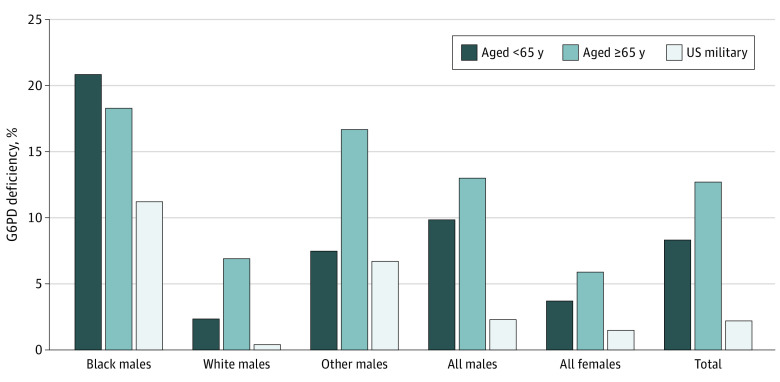
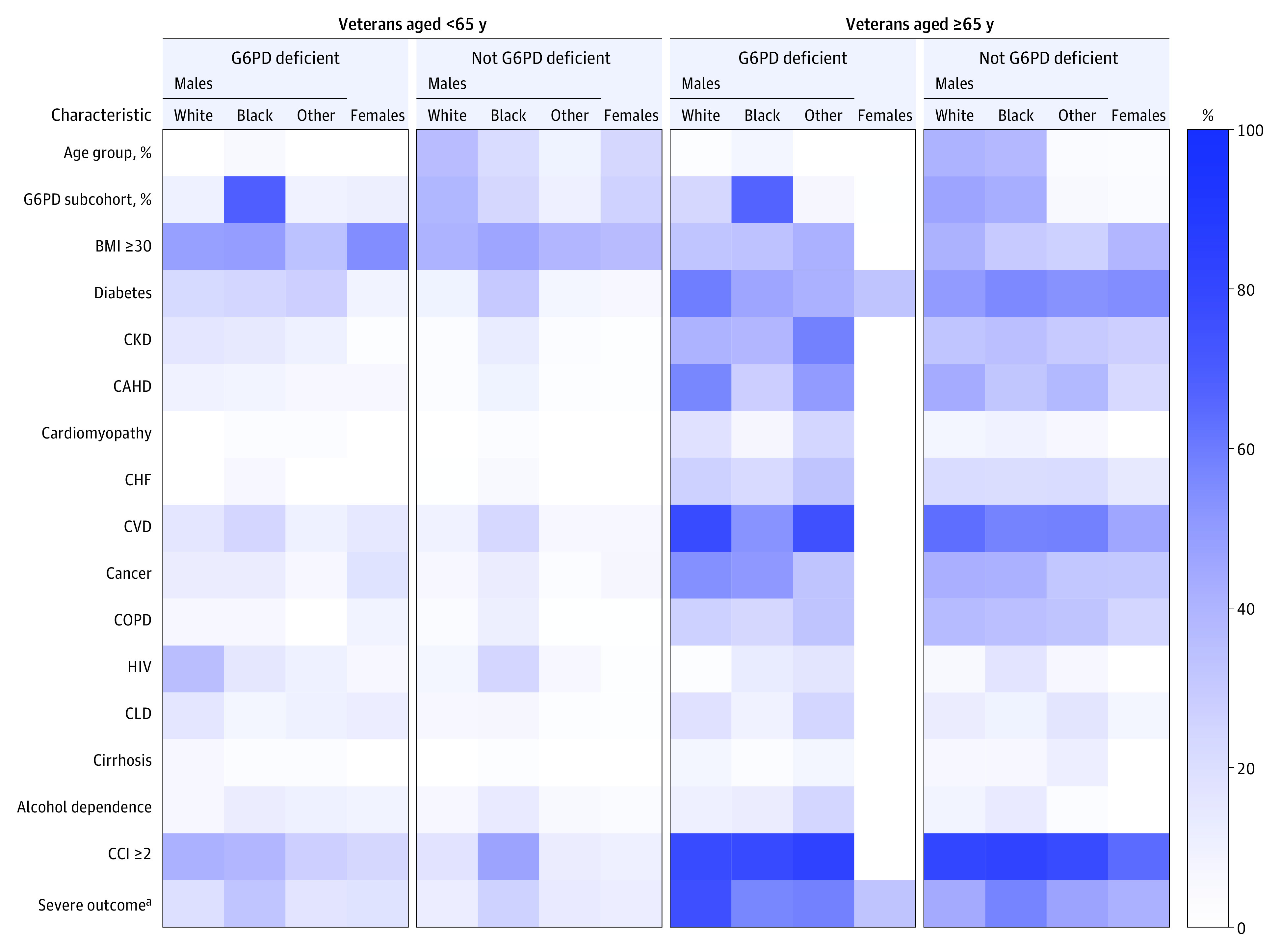
Results: Among 4811 veterans in the Veterans Health Administration who had historical G6PD enzyme activity test results and SARS-CoV-2 positivity included in this study, 3868 (80.4%) were male, 1553 (32.3%) were Black, and 1855 (39%) were White; 1228 (25.5%) were 65 years or older and 3583 (74.5%) were younger than 65 years. There were no significant differences in age, body mass index, or Charlson Comorbidity Index were present between the veterans with G6PD deficiency and without G6PD deficiency. Among these veterans with SARS-CoV-2 infection, G6PD deficiency was more prevalent in Black male veterans (309 of 454 [68.1%]) compared with other racial and ethnic groups. Black male veterans less than 65 years of age with G6PD deficiency had approximately 1.5-fold increased likelihood of developing severe outcomes from SARS-CoV-2 infection compared with Black male veterans without G6PD deficiency (OR, 1.47; 95% CI, 1.03-2.09). In the small subset of White male veterans with G6PD deficiency, we observed an approximately 3.6-fold increased likelihood of developing severe outcomes from SARS-CoV-2 infection compared with White male veterans aged 65 years or older without G6PD deficiency (OR, 3.58; 95% CI, 1.64-7.80). This difference between veterans with and without G6PD deficiency was not observed in younger White male veterans or older Black male veterans, nor in smaller subsets of other male veterans or in female veterans of any age.
Conclusions and relevance: In this cohort study of COVID-19-positive veterans, Black male veterans less than 65 years of age and White male veterans 65 years of age or older with G6PD deficiency had an increased likelihood of developing severe COVID-19 compared with veterans without G6PD deficiency. These data indicate a need to consider the potential for G6PD deficiency prior to treatment of patients with SARS-CoV-2 infection as part of clinical strategies to mitigate severe outcomes.
Conflict of interest statement
Figures
References
-
- Johns Hopkins University & Medicine . COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Accessed September 12, 2021. https://coronavirus.jhu.edu/map.html
-
- World Health Organization . WHO Coronavirus (COVID-19) Dashboard. Accessed September 12, 2021. https://covid19.who.int/
-
- Jain SK, Parsanathan R, Levine SN, Bocchini JA, Holick MF, Vanchiere JA. The potential link between inherited G6PD deficiency, oxidative stress, and vitamin D deficiency and the racial inequities in mortality associated with COVID-19. Free Radic Biol Med. 2020;161:84-91. doi: 10.1016/j.freeradbiomed.2020.10.002 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
