

Postazacitidine clone size predicts long-term outcome of patients with myelodysplastic syndromes and related myeloid neoplasms
- PMID: 36989067
- PMCID: PMC10365941
- DOI: 10.1182/bloodadvances.2022009564
Postazacitidine clone size predicts long-term outcome of patients with myelodysplastic syndromes and related myeloid neoplasms
Abstract
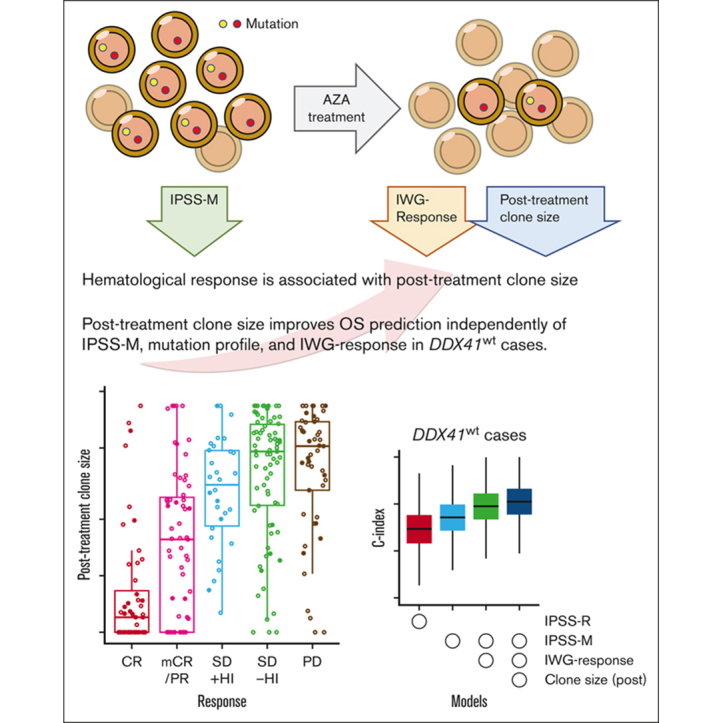
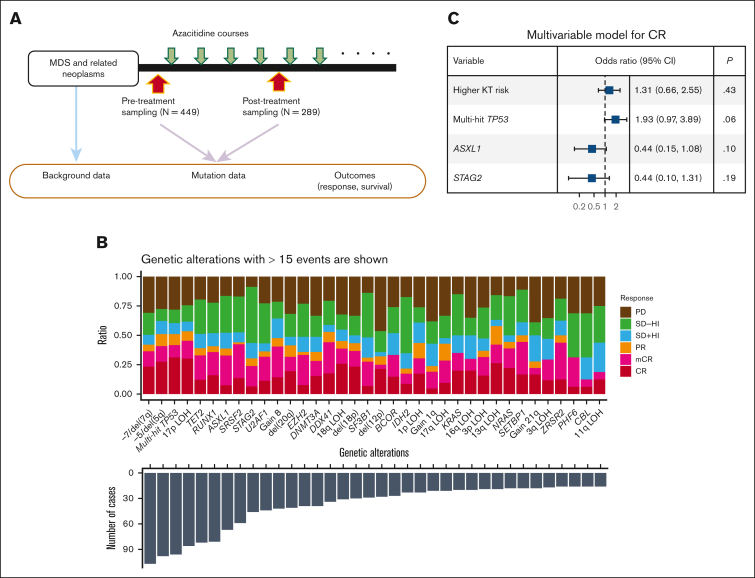
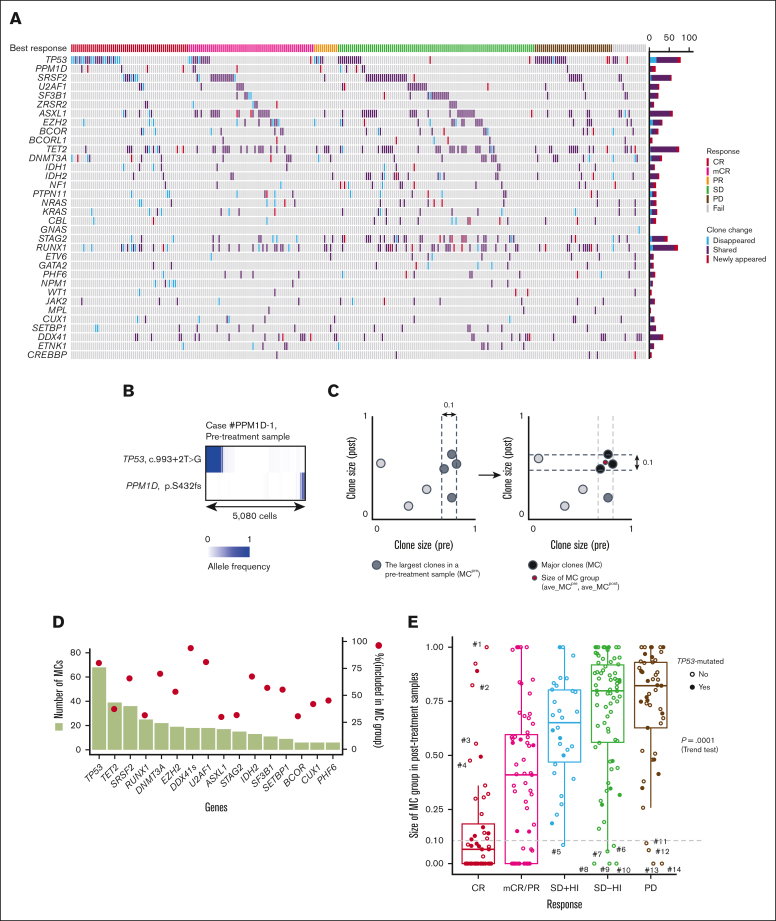
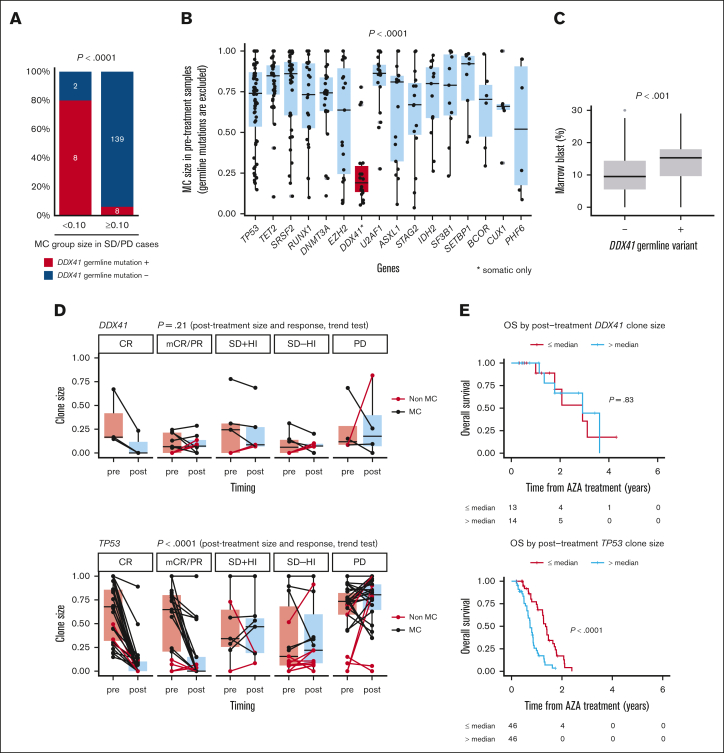
Azacitidine is a mainstay of therapy for myelodysplastic syndrome (MDS)-related diseases. The purpose of our study is to elucidate the effect of gene mutations on hematological response and overall survival (OS), particularly focusing on their posttreatment clone size. We enrolled a total of 449 patients with MDS or related myeloid neoplasms. They were analyzed for gene mutations in pretreatment (n = 449) and posttreatment (n = 289) bone marrow samples using targeted-capture sequencing to assess the impact of gene mutations and their posttreatment clone size on treatment outcomes. In Cox proportional hazard modeling, multihit TP53 mutation (hazard ratio [HR], 2.03; 95% confidence interval [CI], 1.42-2.91; P < .001), EZH2 mutation (HR, 1.71; 95% CI, 1.14-2.54; P = .009), and DDX41 mutation (HR, 0.33; 95% CI, 0.17-0.62; P < .001), together with age, high-risk karyotypes, low platelets, and high blast counts, independently predicted OS. Posttreatment clone size accounting for all drivers significantly correlated with International Working Group (IWG) response (P < .001, using trend test), except for that of DDX41-mutated clones, which did not predict IWG response. Combined, IWG response and posttreatment clone size further improved the prediction of the original model and even that of a recently proposed molecular prediction model, the molecular International Prognostic Scoring System (IPSS-M; c-index, 0.653 vs 0.688; P < .001, using likelihood ratio test). In conclusion, evaluation of posttreatment clone size, together with the pretreatment mutational profile as well as the IWG response play a role in better prognostication of azacitidine-treated patients with myelodysplasia.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: Y.N. reports a consulting or advisory Role at Otsuka Pharmaceutical. K.U. received research funding from Otsuka Pharmaceutical and Nippon Shinyaku; and is on speakers’ bureau at Otsuka Pharmaceutical. K.I. received honoraria from Nippon Shinyaku. T.K. received grants from and is on speakers’ bureau at Nippon Shinyaku. K.O. received honoraria from Nippon Shinyaku. Y.M. received honoraria from Nippon Shinyaku.
Figures


References
-
- Silverman LR, Demakos EP, Peterson BL, et al. Randomized controlled trial of azacitidine in patients with the myelodysplastic syndrome: a study of the cancer and leukemia group B. J Clin Oncol. 2002;20(10):2429–2440. - PubMed
-
- Papageorgiou SG, Vasilatou D, Kontos CK, et al. Treatment with 5-azacytidine improves clinical outcome in high-risk MDS patients in the 'real life' setting: a single center observational study. Hematology. 2016;21(1):34–41. - PubMed
-
- Itzykson R, Kosmider O, Cluzeau T, et al. Impact of TET2 mutations on response rate to azacitidine in myelodysplastic syndromes and low blast count acute myeloid leukemias. Leukemia. 2011;25(7):1147–1152. - PubMed
-
- Itzykson R, Thepot S, Quesnel B, et al. Prognostic factors for response and overall survival in 282 patients with higher-risk myelodysplastic syndromes treated with azacitidine. Blood. 2011;117(2):403–411. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
