

Distinctive serum lipidomic profile of IVIG-resistant Kawasaki disease children before and after treatment
- PMID: 36989310
- PMCID: PMC10057782
- DOI: 10.1371/journal.pone.0283710
Distinctive serum lipidomic profile of IVIG-resistant Kawasaki disease children before and after treatment
Abstract
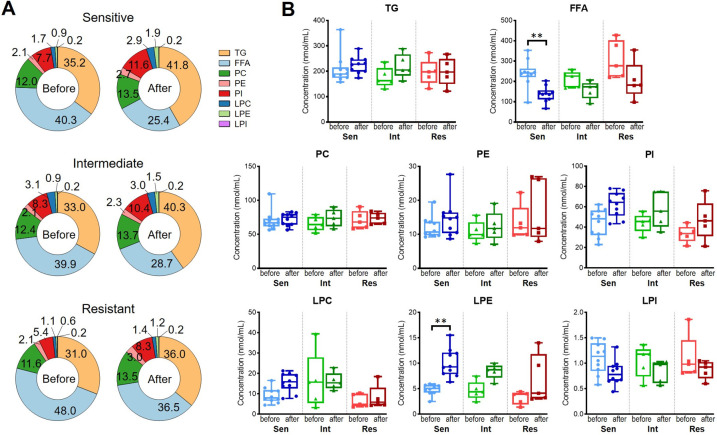
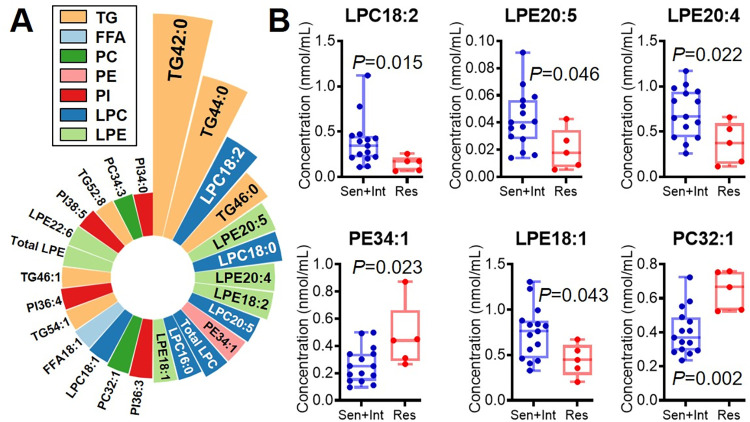
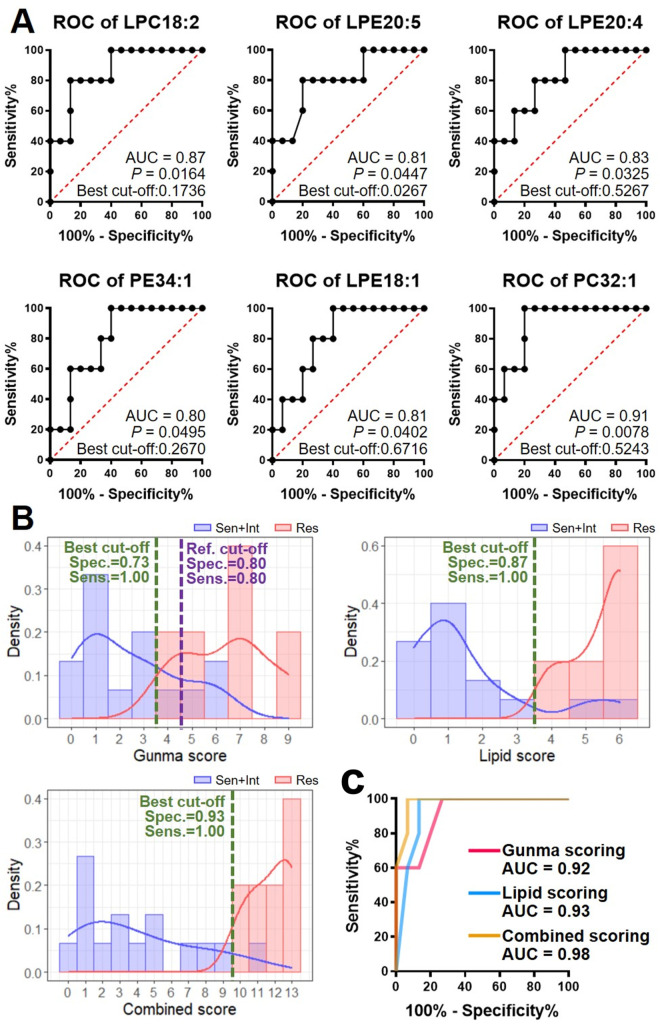
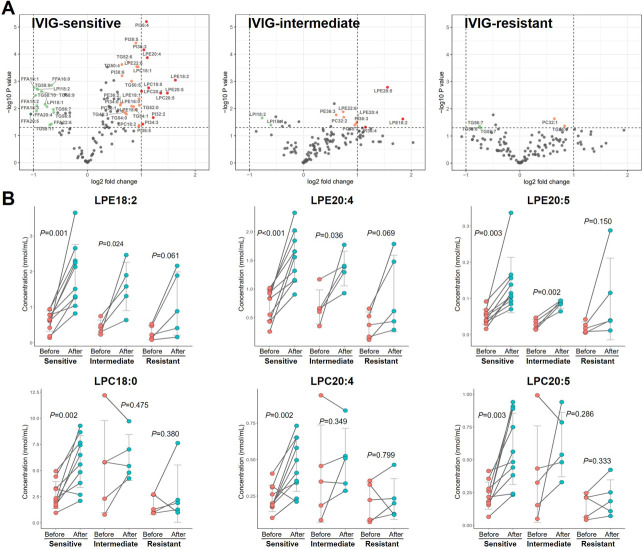
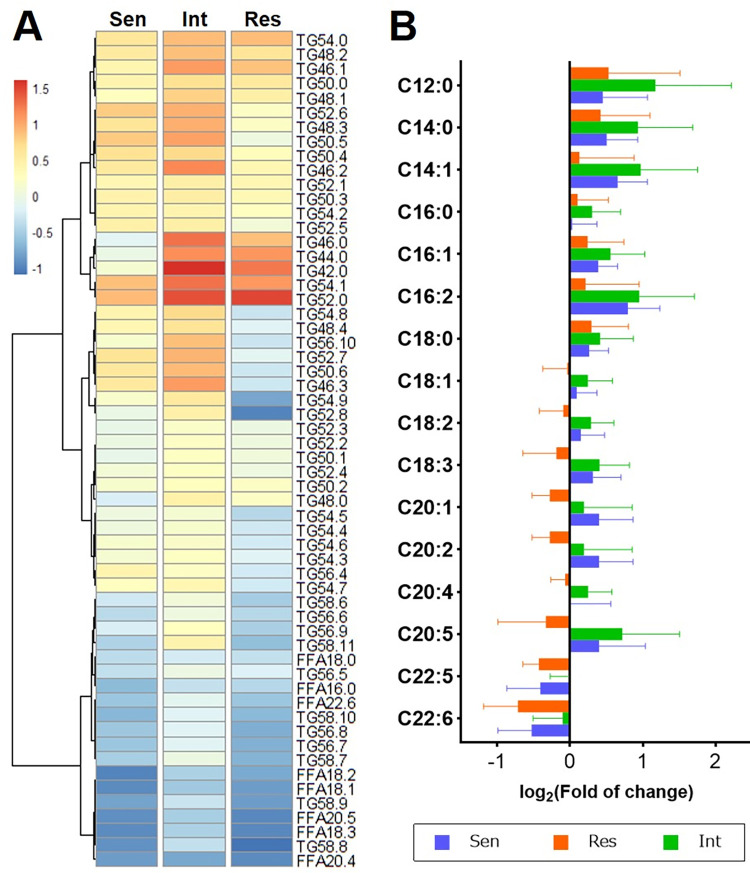
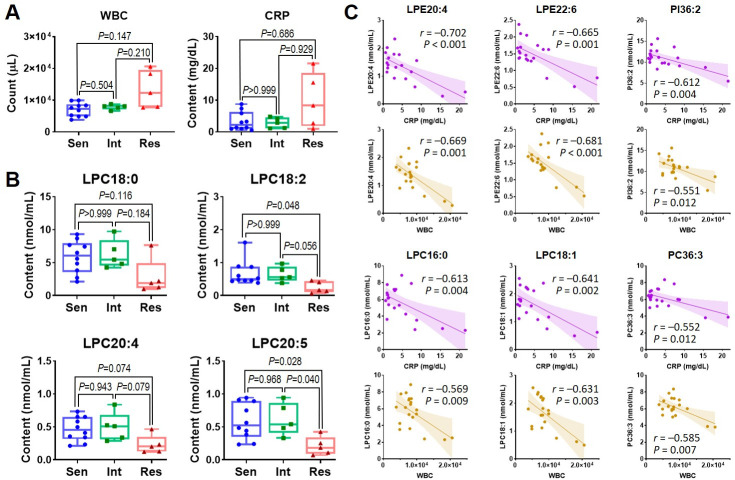
Kawasaki Disease (KD) is an acute inflammatory disorder associated with systemic vasculitis. Intravenous immunoglobulin (IVIG) is an effective therapy for KD, yet, about 20% of cases show IVIG resistance with persistent inflammation. The lipid profile in IVIG-resistant KD patients and the relationship between lipid characteristics and IVIG resistance remain unknown. In this study, serum samples from twenty KD patients with different IVIG responses (sensitive, intermediate, or resistant) were collected both before and after treatment, and lipidomic analysis was performed using high-performance liquid chromatography-mass spectrometry. As a result, before treatment, six lipid species were found as the most variant features, in which all the top decreased lipids in the IVIG-resistant group were lysophosphatidylcholine (LPC) and lysophosphatidylethanolamine (LPE), suggesting the potential to be IVIG-resistant markers in pretreatment diagnosis. During treatment, lipidomic changes showed a weaker response in the IVIG-resistant group. After treatment, LPC and LPE species exhibited lower in the IVIG-resistant group and negative correlation with the inflammatory markers, indicating that the unique metabolism may occur among IVIG-responsiveness. These results might contribute to diagnosing IVIG-resistant patients more accurately for alternative therapy and to a better understanding of how lipid metabolism is associated with IVIG sensitiveness/resistance in KD.
Copyright: © 2023 Chen et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
