

Evaluation and Management of Chronic Thromboembolic Pulmonary Hypertension
- PMID: 36990148
- PMCID: PMC10410247
- DOI: 10.1016/j.chest.2023.03.029
Evaluation and Management of Chronic Thromboembolic Pulmonary Hypertension
Abstract
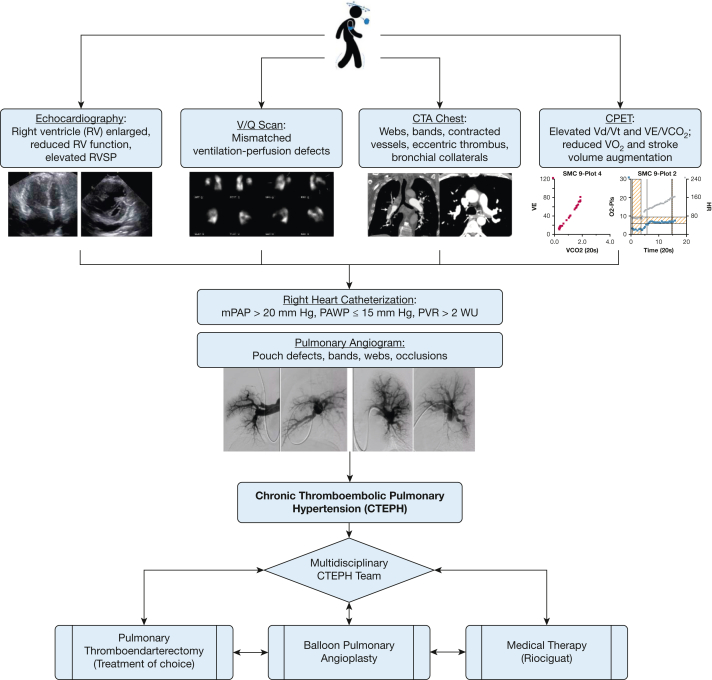
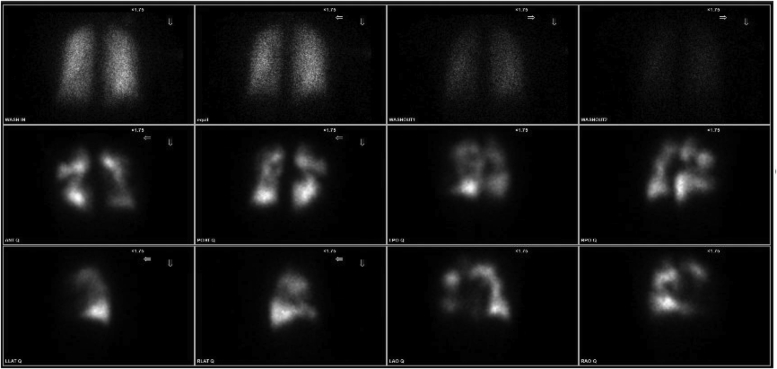
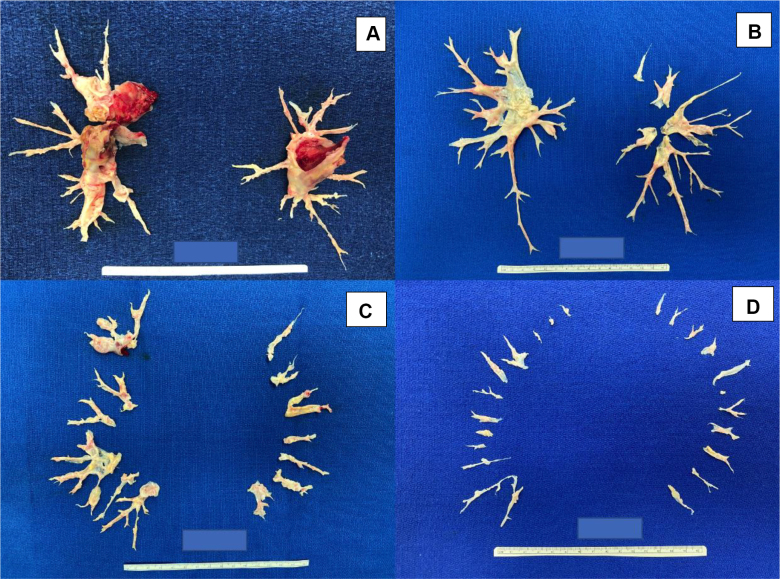
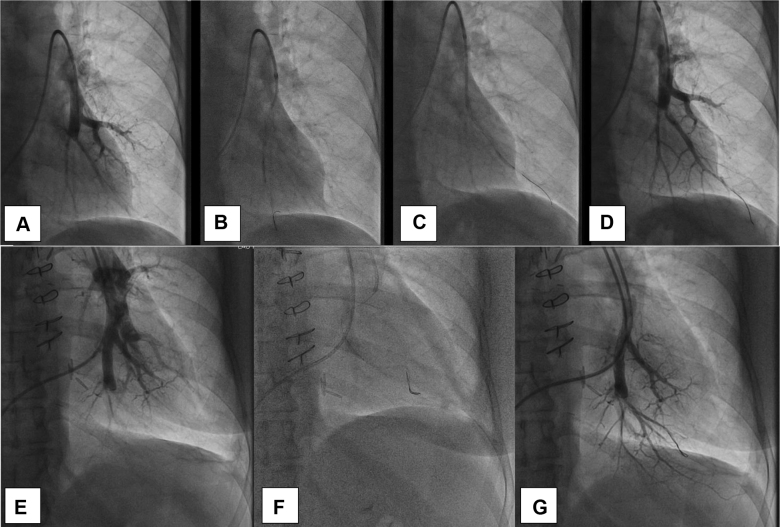
Chronic thromboembolic pulmonary hypertension (CTEPH) is a treatable form of pulmonary hypertension and right heart failure. CTEPH (group 4 pulmonary hypertension) is caused by persistent organized thromboembolic obstruction of the pulmonary arteries from incompletely resolved acute pulmonary embolism. CTEPH also may present without prior VTE history, which can contribute to its underrecognition. The true incidence of CTEPH is unclear, but is estimated to be approximately 3% after acute pulmonary embolism. V˙/Q˙ scintigraphy is the best screening test for CTEPH, with CT scan imaging and other advanced imaging methods now playing a larger role in disease detection and confirmation. Perfusion defects on V˙/Q˙ scintigraphy in the setting of pulmonary hypertension are suggestive of CTEPH, but pulmonary angiography and right heart catheterization are required for confirmation and treatment planning. CTEPH potentially is curative with pulmonary thromboendarterectomy surgery, with mortality rates of approximately 2% at expert centers. Advances in operative techniques are allowing more distal endarterectomies to be performed successfully with favorable outcomes. However, more than one-third of patients may be considered inoperable. Although these patients previously had minimal therapeutic options, effective treatments now are available with pharmacotherapy and balloon pulmonary angioplasty. Diagnosis of CTEPH should be considered in all patients with suspicion of pulmonary hypertension. Treatments for CTEPH have advanced with improvements in outcomes for both operable and inoperable patients. Therapy should be tailored based on multidisciplinary team evaluation to ensure optimal treatment response.
Keywords: Riociguat; balloon pulmonary angioplasty; chronic thromboembolic pulmonary hypertension; pulmonary endarterectomy; pulmonary hypertension.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Delcroix M., Torbicki A., Gopalan D., et al. ERS statement on chronic thromboembolic pulmonary hypertension. Eur Respir J. 2021;57(6) - PubMed
-
- Sanchez O., Helley D., Couchon S., et al. Perfusion defects after pulmonary embolism: risk factors and clinical significance. J Thromb Haemost. 2010;8(6):1248–1255. - PubMed
-
- Pesavento R., Filippi L., Palla A., et al. Impact of residual pulmonary obstruction on the long-term outcome of patients with pulmonary embolism. Eur Respir J. 2017;49(5) - PubMed
-
- Ende-Verhaar Y.M., Cannegieter S.C., Noordegraaf A.V., et al. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: a contemporary view of the published literature. Eur Respir J. 2017;49(2) - PubMed
