

Hematopoietic Somatic Mosaicism Is Associated With an Increased Risk of Postoperative Atrial Fibrillation
- PMID: 36990546
- PMCID: PMC10525908
- DOI: 10.1016/j.jacc.2023.01.036
Hematopoietic Somatic Mosaicism Is Associated With an Increased Risk of Postoperative Atrial Fibrillation
Abstract
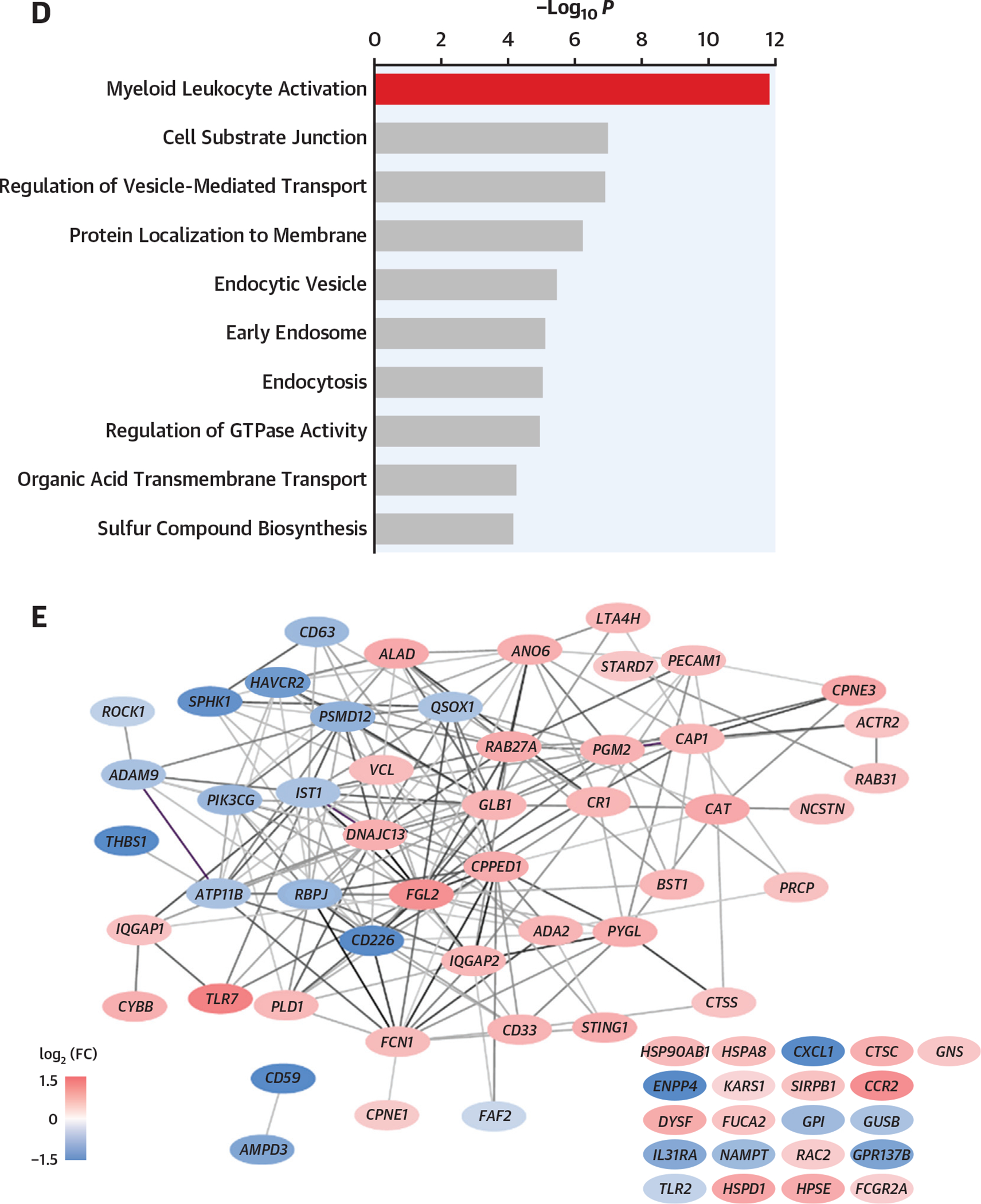
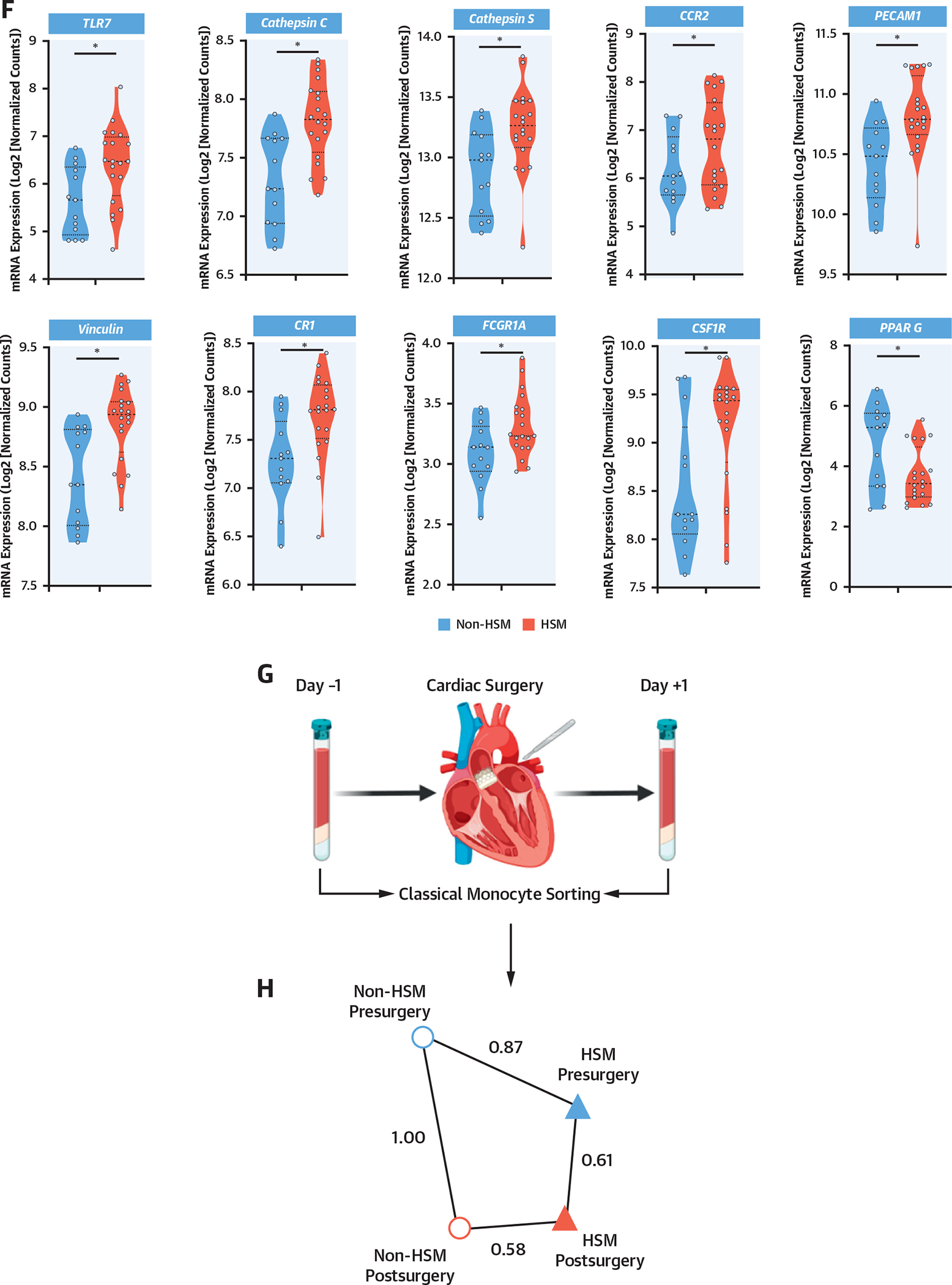
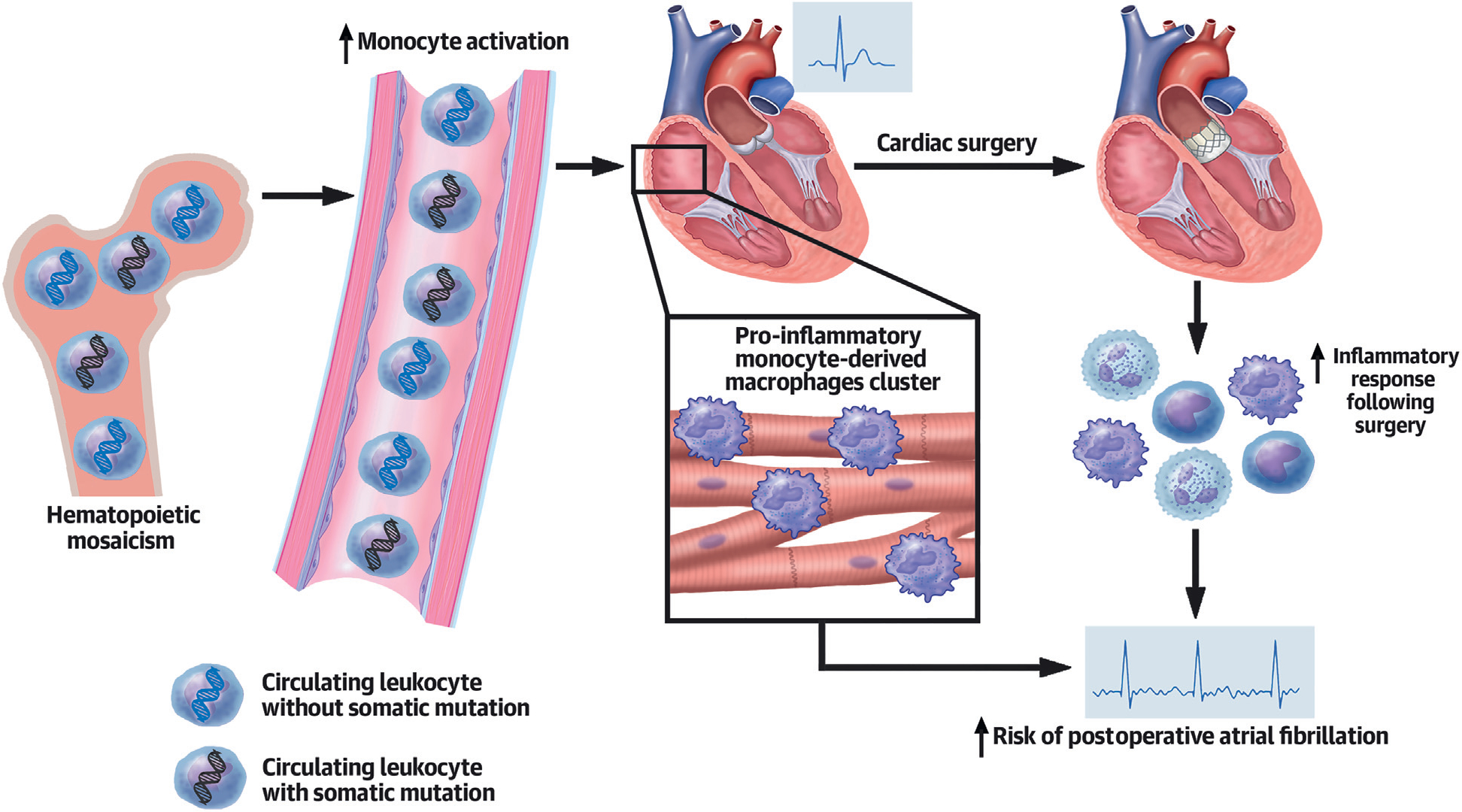
Background: On-pump cardiac surgery triggers sterile inflammation and postoperative complications such as postoperative atrial fibrillation (POAF). Hematopoietic somatic mosaicism (HSM) is a recently identified risk factor for cardiovascular diseases and results in a shift toward a chronic proinflammatory monocyte transcriptome and phenotype.
Objectives: The aim of this study was to assess the prevalence, characteristics, and impact of HSM on preoperative blood and myocardial myeloid cells as well as on outcomes after cardiac surgery.
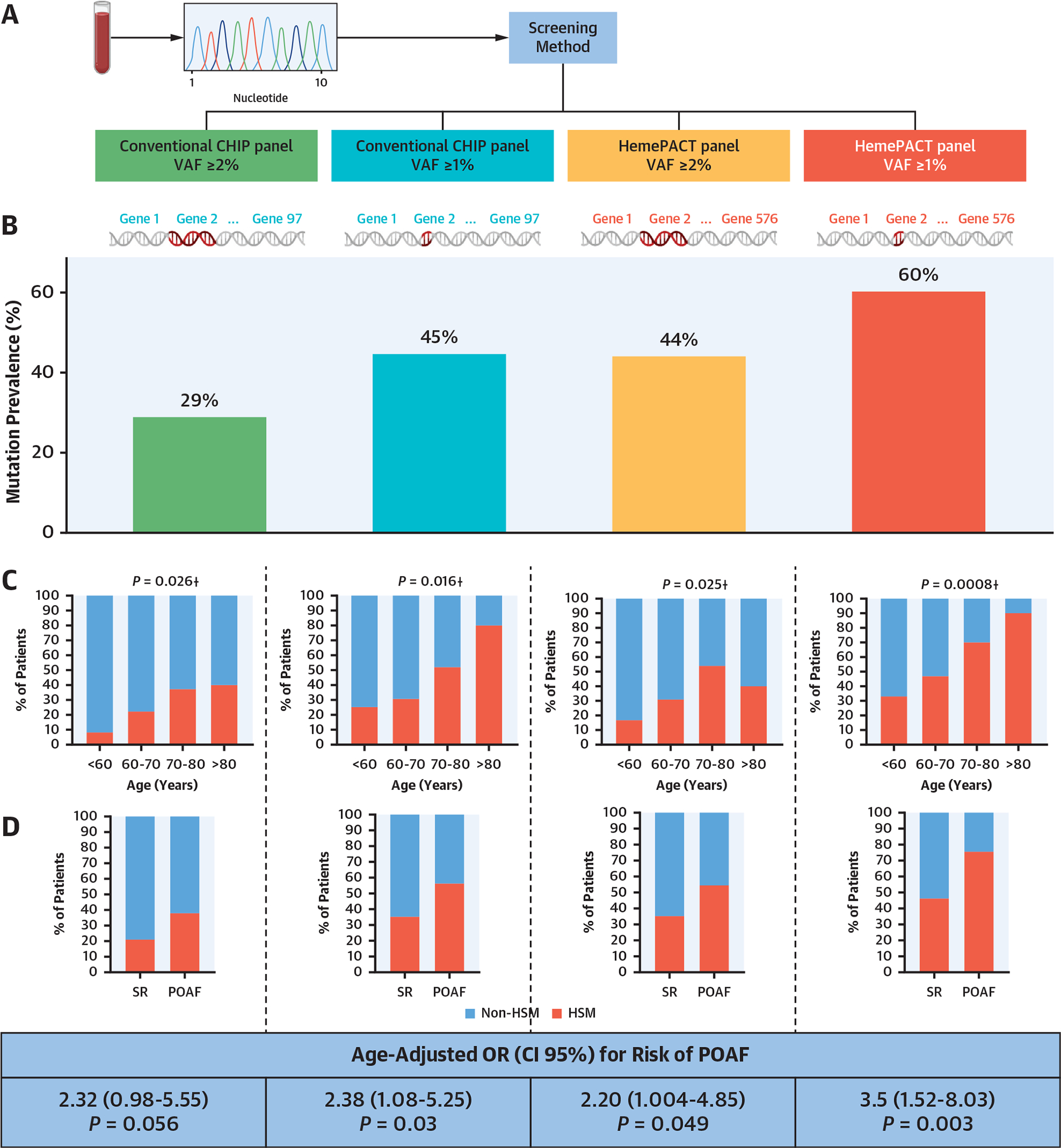
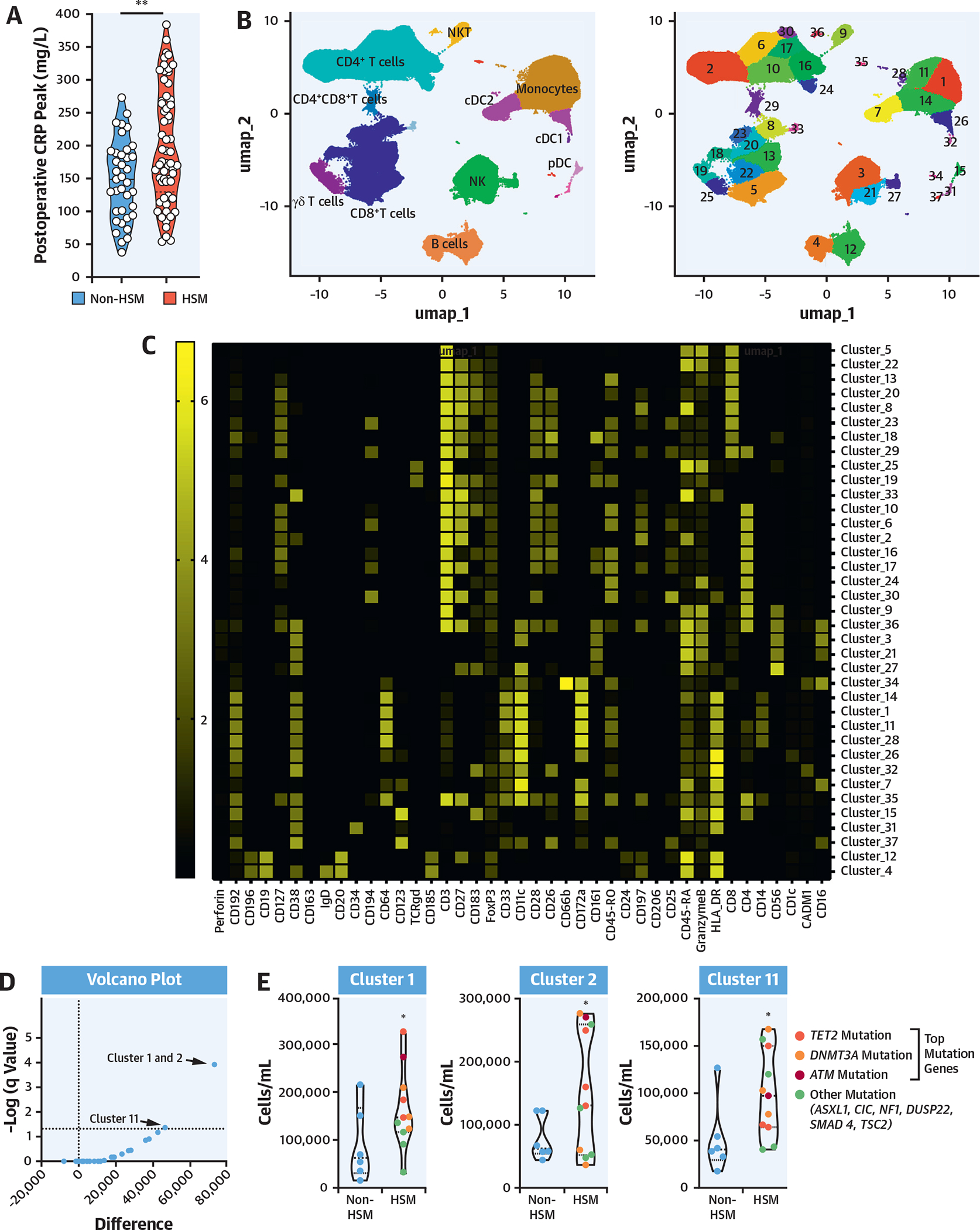
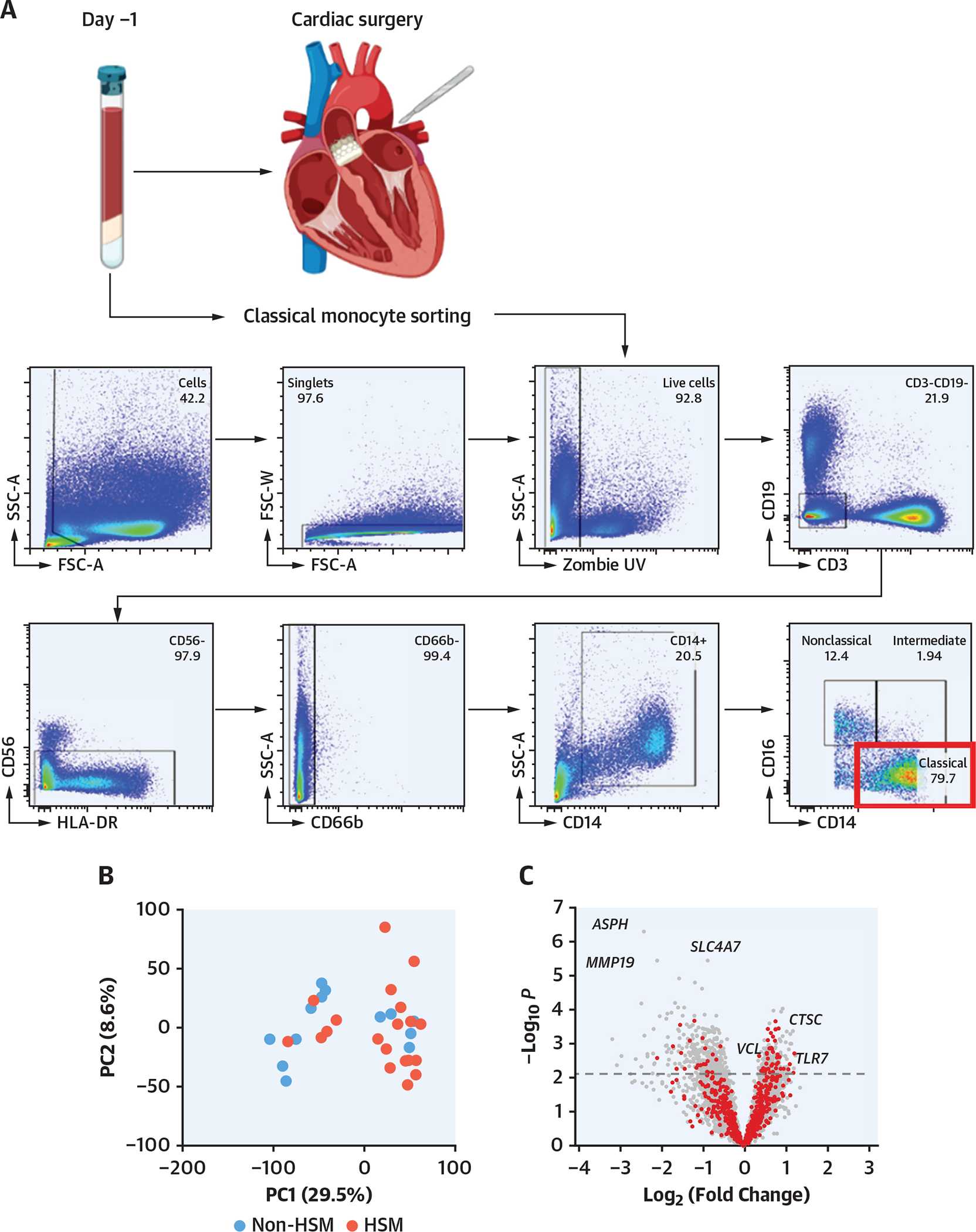
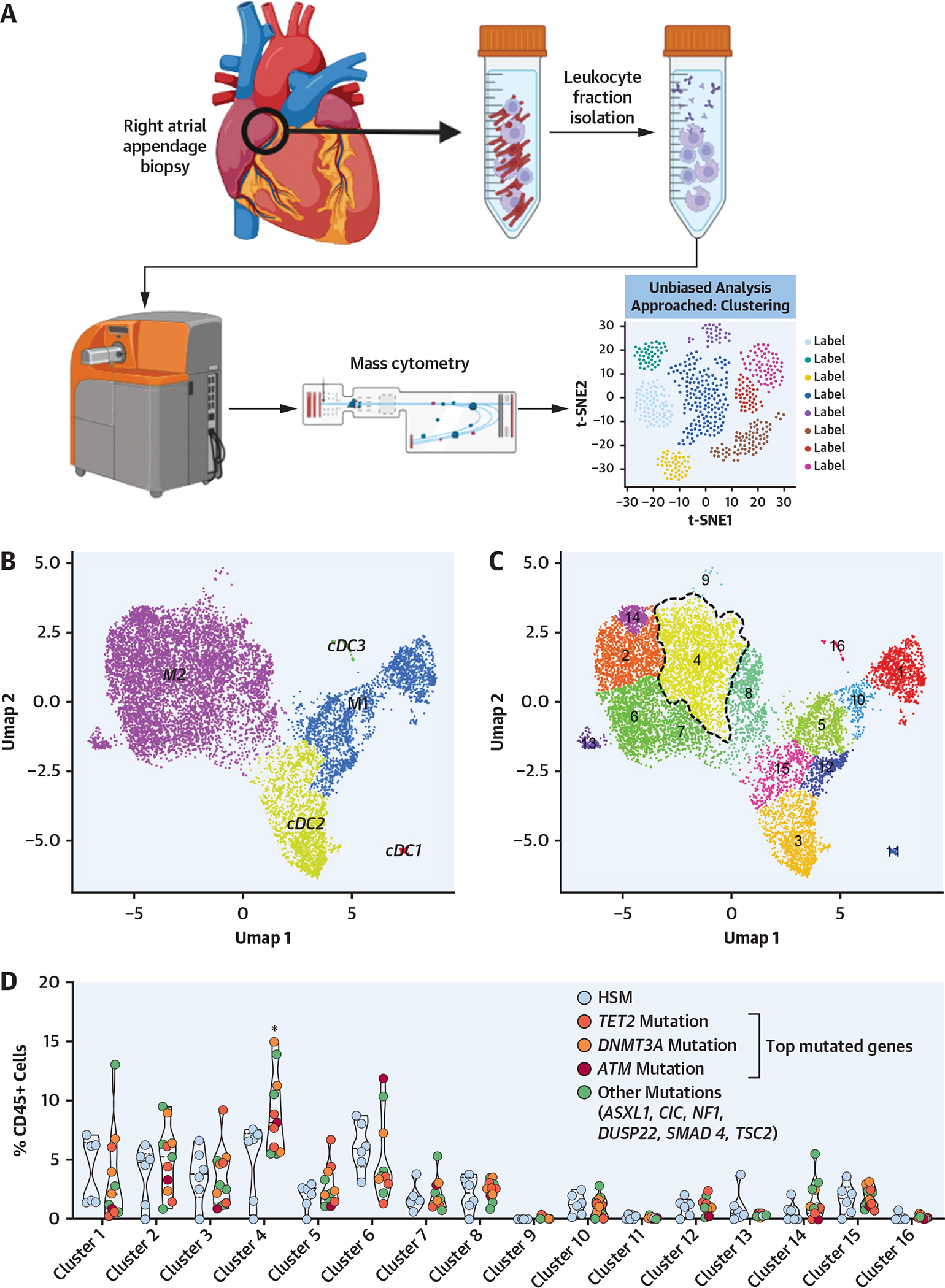
Methods: Blood DNA from 104 patients referred for surgical aortic valve replacement (AVR) was genotyped using the HemePACT panel (576 genes). Four screening methods were applied to assess HSM, and postoperative outcomes were explored. In-depth blood and myocardial leukocyte phenotyping was performed in selected patients using mass cytometry and preoperative and postoperative RNA sequencing analysis of classical monocytes.
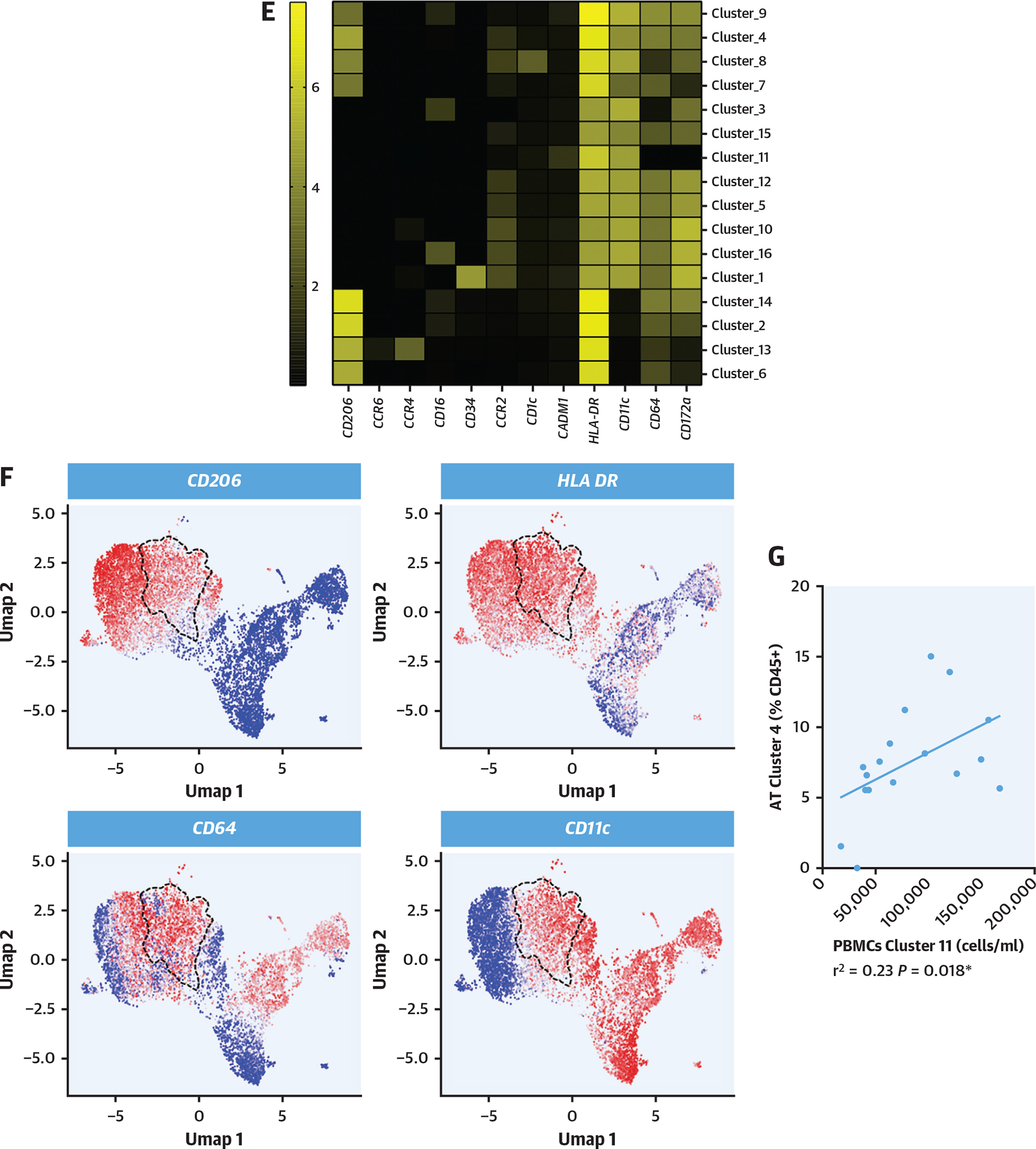
Results: The prevalence of HSM in the patient cohort ranged from 29%, when considering the conventional HSM panel (97 genes) with variant allelic frequencies ≥2%, to 60% when considering the full HemePACT panel and variant allelic frequencies ≥1%. Three of 4 explored HSM definitions were significantly associated with higher risk for POAF. On the basis of the most inclusive definition, HSM carriers exhibited a 3.5-fold higher risk for POAF (age-adjusted OR: 3.5; 95% CI: 1.52-8.03; P = 0.003) and an exaggerated inflammatory response following AVR. HSM carriers presented higher levels of activated CD64+CD14+CD16- circulating monocytes and inflammatory monocyte-derived macrophages in presurgery myocardium.
Conclusions: HSM is frequent in candidates for AVR, is associated with an enrichment of proinflammatory cardiac monocyte-derived macrophages, and predisposes to a higher incidence of POAF. HSM assessment may be useful in the personalized management of patients in the perioperative period. (Post-Operative Myocardial Incident & Atrial Fibrillation [POMI-AF]; NCT03376165).
Keywords: cardiac surgery; clonal hematopoiesis; inflammation; postoperative atrial fibrillation; somatic mosaicism.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by grants from Fédération Française de Cardiologie, Fondation Leducq convention 16CVD01 (“Defining and Targeting Epigenetic Pathways in Monocytes and Macrophages That Contribute to Cardiovascular Disease”), the European Genomic Institute for Diabetes (ANR-10-LABX-0046), Fondation Pour la Recherche Médicale (REFERENCE PROJET EQU202203014650), and Agence Nationale de la Recherche (TOMIS leukocytes: ANR-CE14-0003-01). Dr Staels is a recipient of an Advanced European Research Council Grant (694717). Dr Vicario was supported by the 2018 American Association for Cancer Research–Bristol Myers Squibb Fellowship for Young Investigators in Translational Immuno-Oncology. Work at the Memorial Sloan Kettering Cancer Center (MSKCC) is supported by an MSKCC core grant (P30 CA008748), National Institutes of Health grants 1R01NS115715-01, 1 R01 HL138090-01, and 1 R01 AI130345-01, Basic and Translational Immunology Grants from the Ludwig Center for Cancer Immunotherapy to Dr Geissmann. Dr de Winther is funded by grants from the Netherlands Heart Foundation (CVON: GENIUS2) and the Netherlands Heart Foundation and Spark-Holding (2019B016). Dr Neele is a Dekker fellow of the Netherlands Heart Foundation (2020T029). Dr White is founder and owner of Resphera Biosciences. Dr Geissmann has performed consulting for Third Rock Ventures. Dr Fragkogianni is employed by Tempus Labs. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Fishing CHIPs to Predict Postoperative Atrial Fibrillation.J Am Coll Cardiol. 2023 Apr 4;81(13):1279-1282. doi: 10.1016/j.jacc.2023.01.037. J Am Coll Cardiol. 2023. PMID: 36990547 No abstract available.
References
-
- Dobrev D, Aguilar M, Heijman J, Guichard J-B, Nattel S. Postoperative atrial fibrillation: mechanisms, manifestations and management. Nat Rev Cardiol. 2019;16:417–436. - PubMed
-
- Wang Y, Bellomo R. Cardiac surgery-associated acute kidney injury: risk factors, pathophysiology and treatment. Nat Rev Nephrol. 2017;13:697–711. - PubMed
-
- Wan S, Marchant A, DeSmet JM, et al. Human cytokine responses to cardiac transplantation and coronary artery bypass grafting. J Thorac Cardiovasc Surg. 1996;111:469–477. - PubMed
-
- Gong T, Liu L, Jiang W, Zhou R. DAMP-sensing receptors in sterile inflammation and inflammatory diseases. Nat Rev Immunol. 2020;20:95–112. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
