

Mortality rates of severe COVID-19-related respiratory failure with and without extracorporeal membrane oxygenation in the Middle Ruhr Region of Germany
- PMID: 36991018
- PMCID: PMC10054204
- DOI: 10.1038/s41598-023-31944-7
Mortality rates of severe COVID-19-related respiratory failure with and without extracorporeal membrane oxygenation in the Middle Ruhr Region of Germany
Erratum in
-
Publisher Correction: Mortality rates of severe COVID-19-related respiratory failure with and without extracorporeal membrane oxygenation in the Middle Ruhr Region of Germany.Sci Rep. 2023 Apr 20;13(1):6442. doi: 10.1038/s41598-023-33475-7. Sci Rep. 2023. PMID: 37081059 Free PMC article. No abstract available.
Abstract
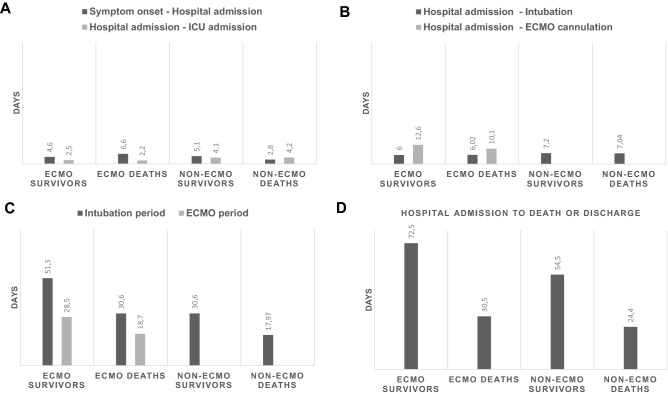
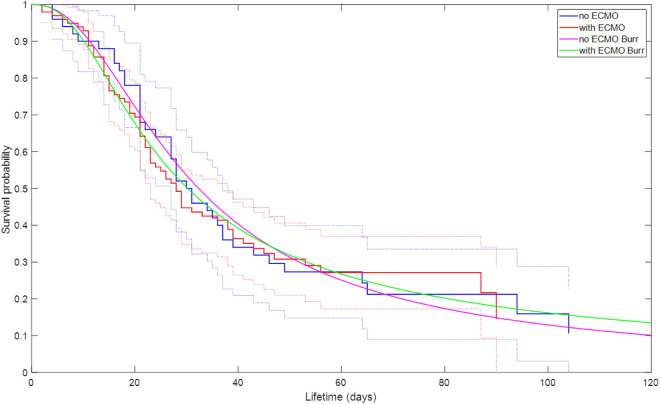
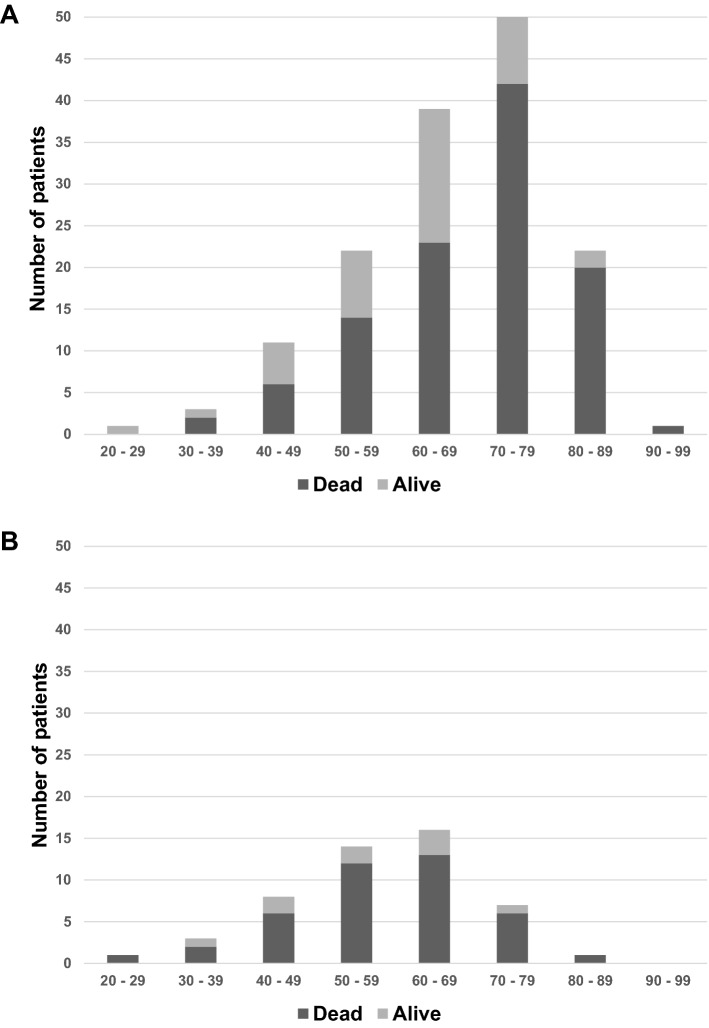
The use of extracorporeal membrane oxygenation (ECMO) is discussed to improve patients' outcome in severe COVID-19 with respiratory failure, but data on ECMO remains controversial. The aim of the study was to determine the characteristics of patients under invasive mechanical ventilation (IMV) with or without veno-venous ECMO support and to evaluate outcome parameters. Ventilated patients with COVID-19 with and without additional ECMO support were analyzed in a retrospective multicenter study regarding clinical characteristics, respiratory and laboratory parameters in day-to-day follow-up. Recruitment of patients was conducted during the first three COVID-19 waves at four German university hospitals of the Ruhr University Bochum, located in the Middle Ruhr Region. From March 1, 2020 to August 31, 2021, the charts of 149 patients who were ventilated for COVID-19 infection, were included (63.8% male, median age 67 years). Fifty patients (33.6%) received additional ECMO support. On average, ECMO therapy was initiated 15.6 ± 9.4 days after symptom onset, 10.6 ± 7.1 days after hospital admission, and 4.8 ± 6.4 days after the start of IMV. Male sex and higher SOFA and RESP scores were observed significantly more often in the high-volume ECMO center. Pre-medication with antidepressants was more often detected in survivors (22.0% vs. 6.5%; p = 0.006). ECMO patients were 14 years younger and presented a lower rate of concomitant cardiovascular diseases (18.0% vs. 47.5%; p = 0.0004). Additionally, cytokine-adsorption (46.0% vs. 13.1%; p < 0.0001) and renal replacement therapy (76.0% vs. 43.4%; p = 0.0001) were carried out more frequently; in ECMO patients thrombocytes were transfused 12-fold more often related to more than fourfold higher bleeding complications. Undulating C-reactive protein (CRP) and massive increase in bilirubin levels (at terminal stage) could be observed in deceased ECMO patients. In-hospital mortality was high (Overall: 72.5%, ECMO: 80.0%, ns). Regardless of ECMO therapy half of the study population deceased within 30 days after hospital admission. Despite being younger and with less comorbidities ECMO therapy did not improve survival in severely ill COVID-19 patients. Undulating CRP levels, a massive increase of bilirubin level and a high use of cytokine-adsorption were associated with worse outcomes. In conclusion, ECMO support might be helpful in selected severe cases of COVID-19.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Osuchowski MF, Winkler MS, Skirecki T, Cajander S, Shankar-Hari M, Lachmann G, Monneret G, Venet F, Bauer M, Brunkhorst FM, Weis S, Garcia-Salido A, Kox M, Cavaillon JM, Uhle F, Weigand MA, Flohé SB, Wiersinga WJ, Almansa R, de la Fuente A, Martin-Loeches I, Meisel C, Spinetti T, Schefold JC, Cilloniz C, Torres A, Giamarellos-Bourboulis EJ, Ferrer R, Girardis M, Cossarizza A, Netea MG, van der Poll T, Bermejo-Martín JF, Rubio I. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir Med. 2021;9(6):622–642. doi: 10.1016/S2213-2600(21)00218-6. - DOI - PMC - PubMed
-
- Nicholson CJ, Wooster L, Sigurslid HH, Li RH, Jiang W, Tian W, Lino Cardenas CL, Malhotra R. Estimating risk of mechanical ventilation and in-hospital mortality among adult COVID-19 patients admitted to Mass General Brigham: The VICE and DICE scores. EClinicalMedicine. 2021;33:100765. doi: 10.1016/j.eclinm.2021.100765. - DOI - PMC - PubMed
-
- Alshahrani MS, Sindi A, Alshamsi F, Al-Omari A, El Tahan M, Alahmadi B, Zein A, Khatani N, Al-Hameed F, Alamri S, Abdelzaher M, Alghamdi A, Alfousan F, Tash A, Tashkandi W, Alraddadi R, Lewis K, Badawee M, Arabi YM, Fan E, Alhazzani W. Extracorporeal membrane oxygenation for severe Middle East respiratory syndrome coronavirus. Ann. Intensive Care. 2018;8(1):3. doi: 10.1186/s13613-017-0350-x.PMID:29330690;PMCID:PMC5768582. - DOI - PMC - PubMed
-
- Fraaij PL, Wildschut ED, Houmes RJ, et al. Severe acute respiratory infection caused by swine influenza virus in a child necessitating extracorporeal membrane oxygenation (ECMO), the Netherlands, October 2016. Eurosurveill. 2016;21:30416. doi: 10.2807/1560-7917.ES.2016.21.48.30416. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
