

The co-development of a linguistic and culturally tailored tele-retinopathy screening intervention for immigrants living with diabetes from China and African-Caribbean countries in Ottawa, Canada
- PMID: 36991464
- PMCID: PMC10054218
- DOI: 10.1186/s12913-023-09329-3
The co-development of a linguistic and culturally tailored tele-retinopathy screening intervention for immigrants living with diabetes from China and African-Caribbean countries in Ottawa, Canada
Abstract
Background: Diabetic retinopathy is a sight-threatening ocular complication of diabetes. Screening is an effective way to reduce severe complications, but screening attendance rates are often low, particularly for newcomers and immigrants to Canada and people from cultural and linguistic minority groups. Building on previous work, in partnership with patient and health system stakeholders, we co-developed a linguistically and culturally tailored tele-retinopathy screening intervention for people living with diabetes who recently immigrated to Canada from either China or African-Caribbean countries.
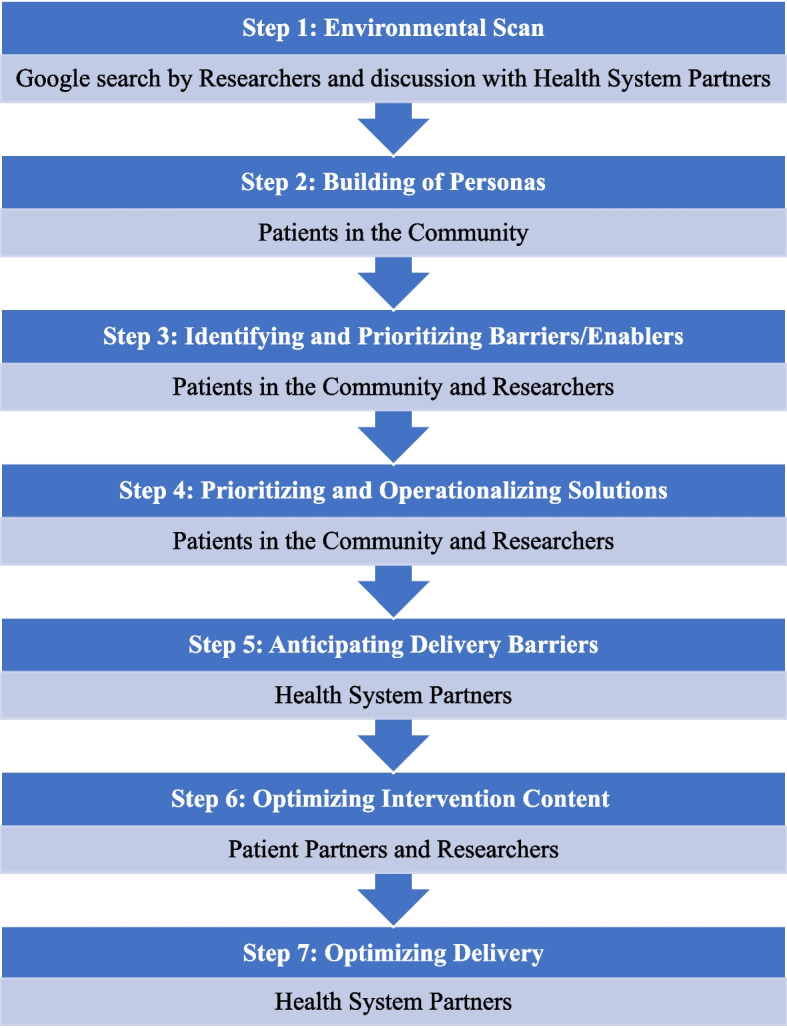
Methods: Following an environmental scan of diabetes eye care pathways in Ottawa, we conducted co-development workshops using a nominal group technique to create and prioritize personas of individuals requiring screening and identify barriers to screening that each persona may face. Next, we used the Theoretical Domains Framework to categorize the barriers/enablers and then mapped these categories to potential evidence-informed behaviour change techniques. Finally with these techniques in mind, participants prioritized strategies and channels of delivery, developed intervention content, and clarified actions required by different actors to overcome anticipated intervention delivery barriers.
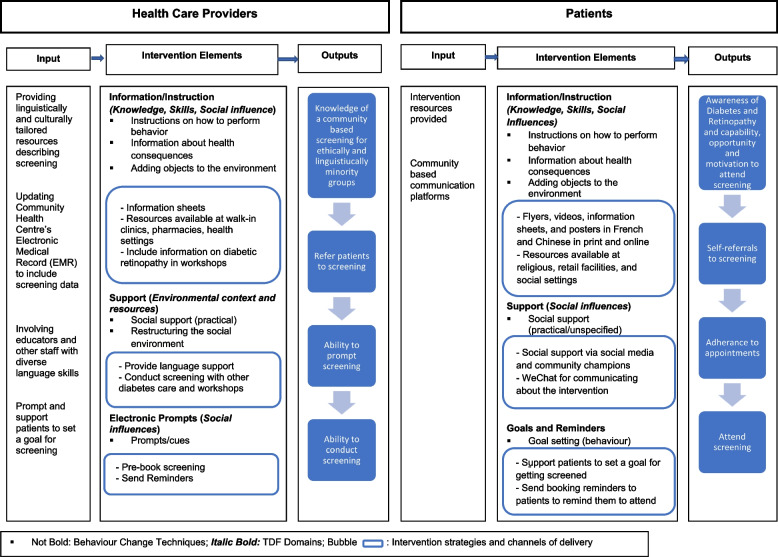
Results: We carried out iterative co-development workshops with Mandarin and French-speaking individuals living with diabetes (i.e., patients in the community) who immigrated to Canada from China and African-Caribbean countries (n = 13), patient partners (n = 7), and health system partners (n = 6) recruited from community health centres in Ottawa. Patients in the community co-development workshops were conducted in Mandarin or French. Together, we prioritized five barriers to attending diabetic retinopathy screening: language (TDF Domains: skills, social influences), retinopathy familiarity (knowledge, beliefs about consequences), physician barriers regarding communication for screening (social influences), lack of publicity about screening (knowledge, environmental context and resources), and fitting screening around other activities (environmental context and resources). The resulting intervention included the following behaviour change techniques to address prioritized local barriers: information about health consequence, providing instructions on how to attend screening, prompts/cues, adding objects to the environment, social support, and restructuring the social environment. Operationalized delivery channels incorporated language support, pre-booking screening and sending reminders, social support via social media and community champions, and providing using flyers and videos as delivery channels.
Conclusion: Working with intervention users and stakeholders, we co-developed a culturally and linguistically relevant tele-retinopathy intervention to address barriers to attending diabetic retinopathy screening and increase uptake among two under-served groups.
Keywords: Diabetic Retinopathy; Health services; Intervention development; Patient Involvement; Patient oriented research; Retinal Screening; Stakeholder consultation; Tele-retinopathy; Theoretical Domains Framework.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hooper P, Boucher MC, Cruess A, Dawson KG, Delpero W, Greve M, et al. Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of diabetic retinopathy. Canadian Journal of Ophthalmology / Journal Canadien d’Ophtalmologie. 2012;47(2):S1–30. doi: 10.1016/j.jcjo.2011.12.025. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
