

Intraoperative Beat-to-Beat Pulse Transit Time (PTT) Monitoring via Non-Invasive Piezoelectric/Piezocapacitive Peripheral Sensors Can Predict Changes in Invasively Acquired Blood Pressure in High-Risk Surgical Patients
- PMID: 36992016
- PMCID: PMC10059272
- DOI: 10.3390/s23063304
Intraoperative Beat-to-Beat Pulse Transit Time (PTT) Monitoring via Non-Invasive Piezoelectric/Piezocapacitive Peripheral Sensors Can Predict Changes in Invasively Acquired Blood Pressure in High-Risk Surgical Patients
Abstract
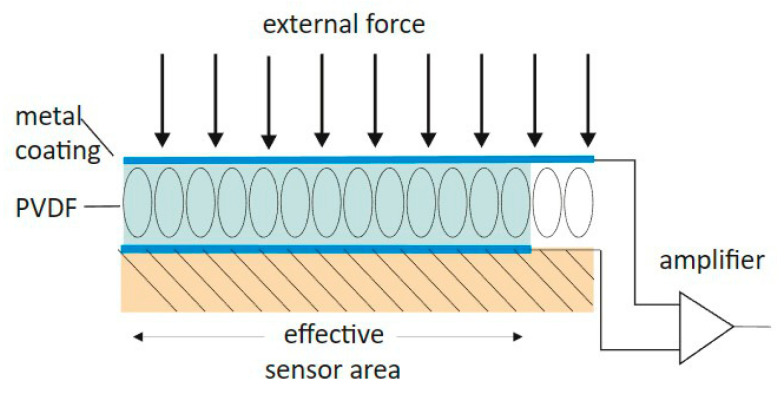
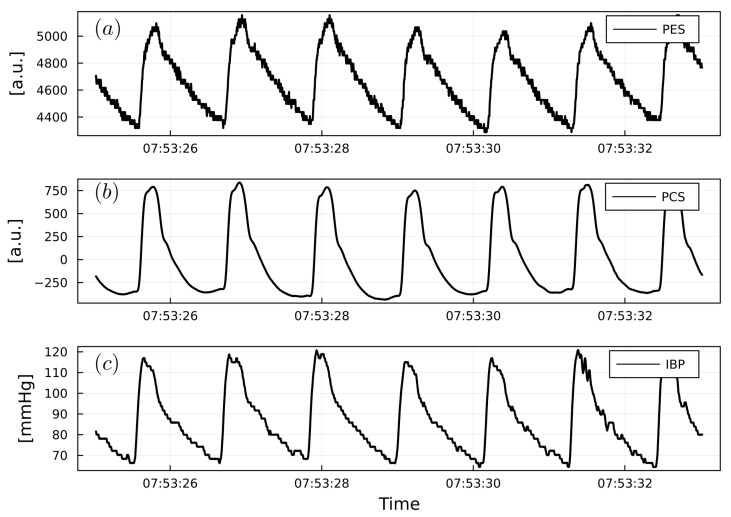
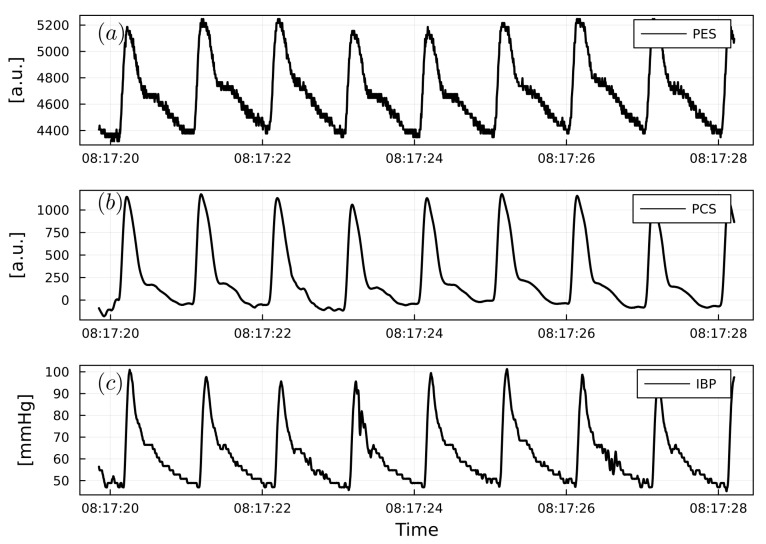
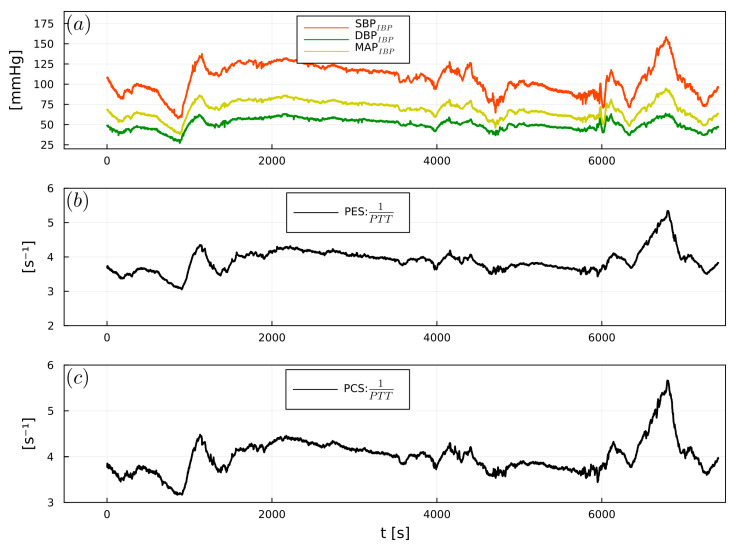
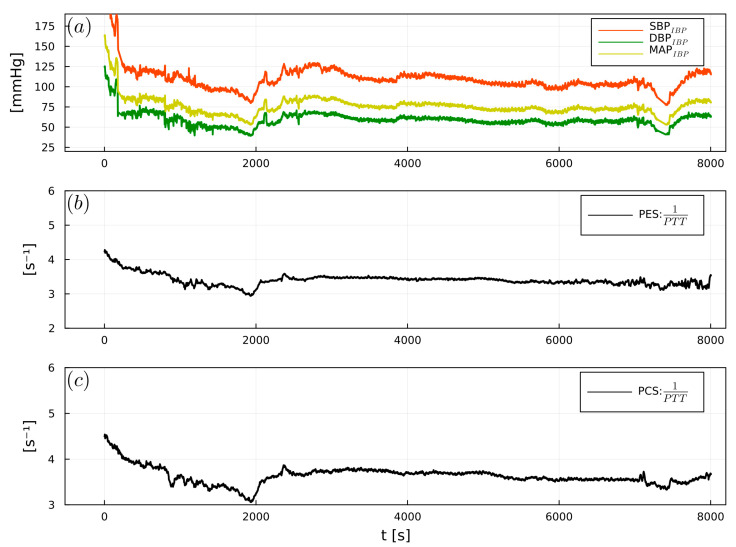
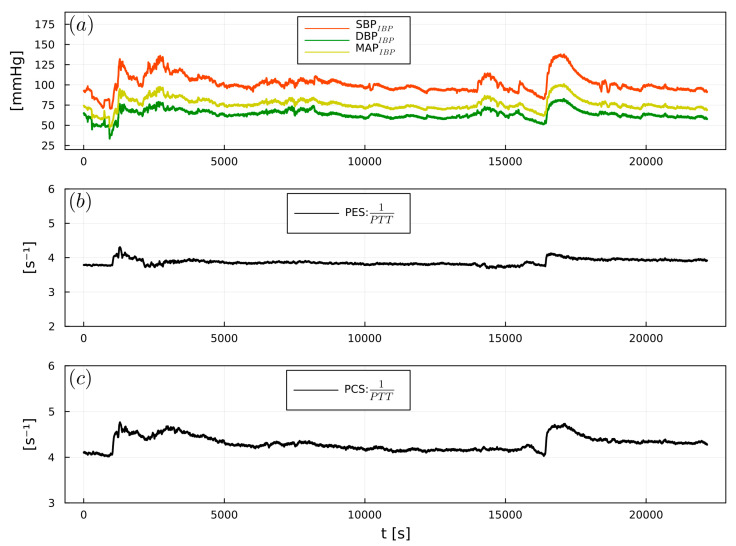
Background: Non-invasive tracking of beat-to-beat pulse transit time (PTT) via piezoelectric/piezocapacitive sensors (PES/PCS) may expand perioperative hemodynamic monitoring. This study evaluated the ability for PTT via PES/PCS to correlate with systolic, diastolic, and mean invasive blood pressure (SBPIBP, DBPIBP, and MAPIBP, respectively) and to detect SBPIBP fluctuations.
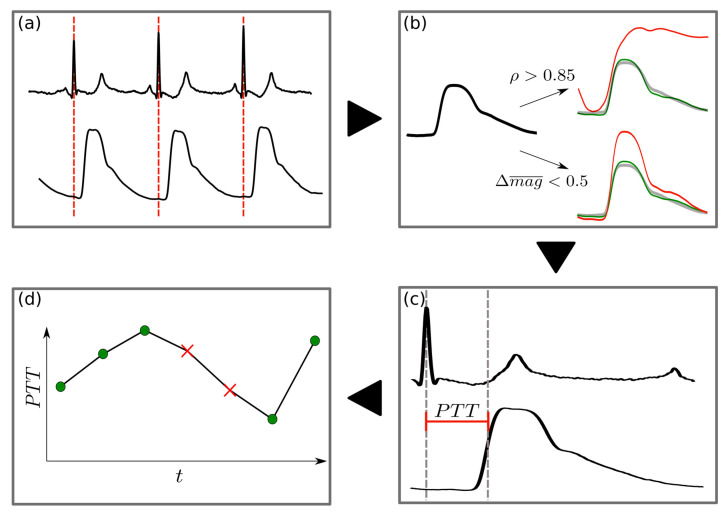
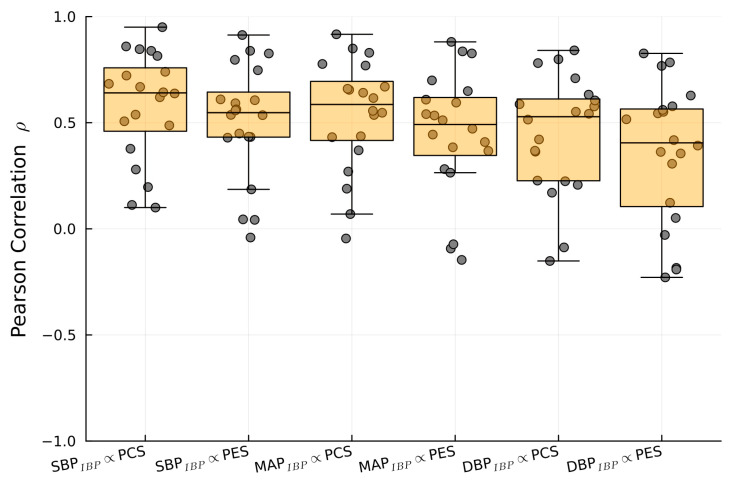
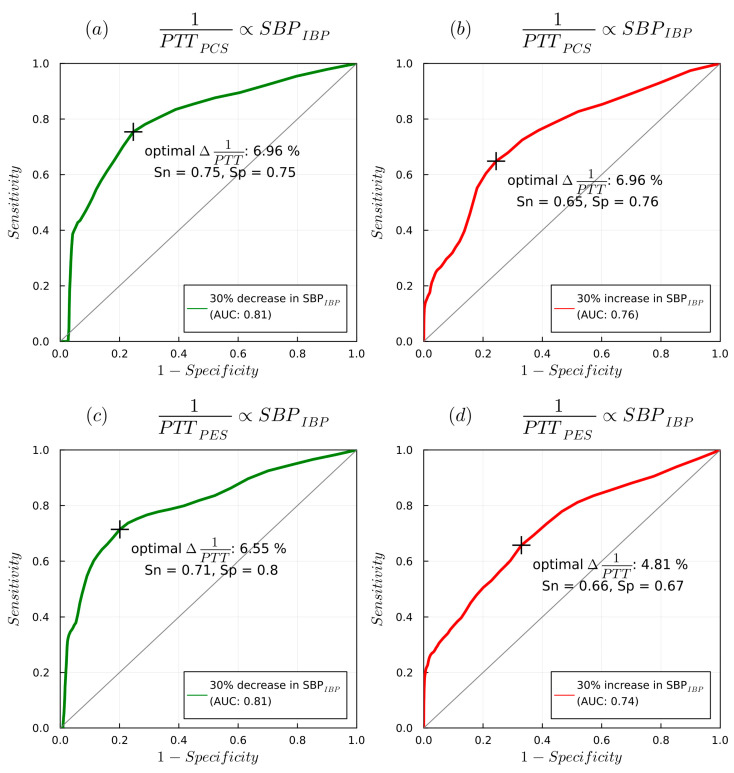
Methods: PES/PCS and IBP measurements were performed in 20 patients undergoing abdominal, urological, and cardiac surgery. A Pearson's correlation analysis (r) between 1/PTT and IBP was performed. The predictive ability of 1/PTT with changes in SBPIBP was determined by area under the curve (reported as AUC, sensitivity, specificity).
Results: Significant correlations between 1/PTT and SBPIBP were found for PES (r = 0.64) and PCS (r = 0.55) (p < 0.01), as well as MAPIBP/DBPIBP for PES (r = 0.6/0.55) and PCS (r = 0.5/0.45) (p < 0.05). A 7% decrease in 1/PTTPES predicted a 30% SBPIBP decrease (0.82, 0.76, 0.76), while a 5.6% increase predicted a 30% SBPIBP increase (0.75, 0.7, 0.68). A 6.6% decrease in 1/PTTPCS detected a 30% SBPIBP decrease (0.81, 0.72, 0.8), while a 4.8% 1/PTTPCS increase detected a 30% SBPIBP increase (0.73, 0.64, 0.68).
Conclusions: Non-invasive beat-to-beat PTT via PES/PCS demonstrated significant correlations with IBP and detected significant changes in SBPIBP. Thus, PES/PCS as a novel sensor technology may augment intraoperative hemodynamic monitoring during major surgery.
Keywords: anesthesiology; intraoperative blood pressure; non-invasive hemodynamics; piezocapacitive; piezoelectric; pulse transit time.
Conflict of interest statement
RFT has received funding from Deutsche Herzstiftung (German Heart Foundation) and DZHK (German Centre for Cardiovascular Research). MN, MP, JK, CB, PB, and NW report no conflict of interest. RK and PK work for SectorCon-Ingenieurgesellschaft mbH, Berlin, Germany, and had no role in the final conclusions derived from this research. ST received funding for experimental research as well as honoraria for lectures from Edwards, Orion Pharma, Amomed, Cytosorbents, Philips, and Smith & Nephews, outside this work.
Figures


Similar articles
-
Beat-to-beat tracking of systolic blood pressure using noninvasive pulse transit time during anesthesia induction in hypertensive patients.Anesth Analg. 2013 Jan;116(1):94-100. doi: 10.1213/ANE.0b013e318270a6d9. Epub 2012 Dec 7. Anesth Analg. 2013. PMID: 23223109
-
Assessment of pulse transit time to indicate cardiovascular changes during obstetric spinal anaesthesia.Br J Anaesth. 2006 Jan;96(1):100-5. doi: 10.1093/bja/aei266. Epub 2005 Oct 28. Br J Anaesth. 2006. PMID: 16257996
-
Comparison of noninvasive pulse transit time estimates as markers of blood pressure using invasive pulse transit time measurements as a reference.Physiol Rep. 2016 May;4(10):e12768. doi: 10.14814/phy2.12768. Physiol Rep. 2016. PMID: 27233300 Free PMC article.
-
Continuous cuffless and non-invasive measurement of arterial blood pressure-concepts and future perspectives.Blood Press. 2022 Dec;31(1):254-269. doi: 10.1080/08037051.2022.2128716. Blood Press. 2022. PMID: 36184775 Review.
-
Blood pressure wave propagation-a multisensor setup for cerebral autoregulation studies.Physiol Meas. 2021 Dec 28;42(11). doi: 10.1088/1361-6579/ac3629. Physiol Meas. 2021. PMID: 34731844 Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
