

Quantifying States and Transitions of Emerging Postural Control for Children Not Yet Able to Sit Independently
- PMID: 36992020
- PMCID: PMC10054170
- DOI: 10.3390/s23063309
Quantifying States and Transitions of Emerging Postural Control for Children Not Yet Able to Sit Independently
Abstract
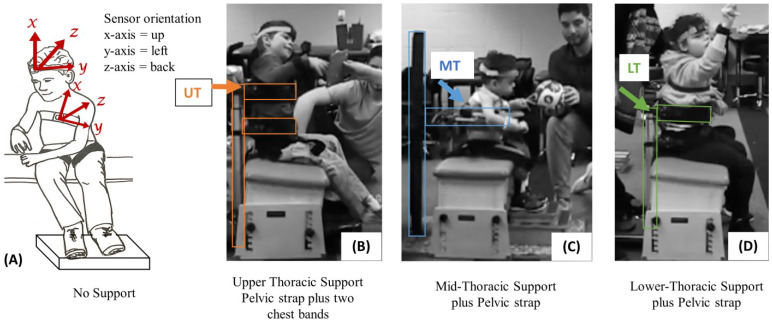
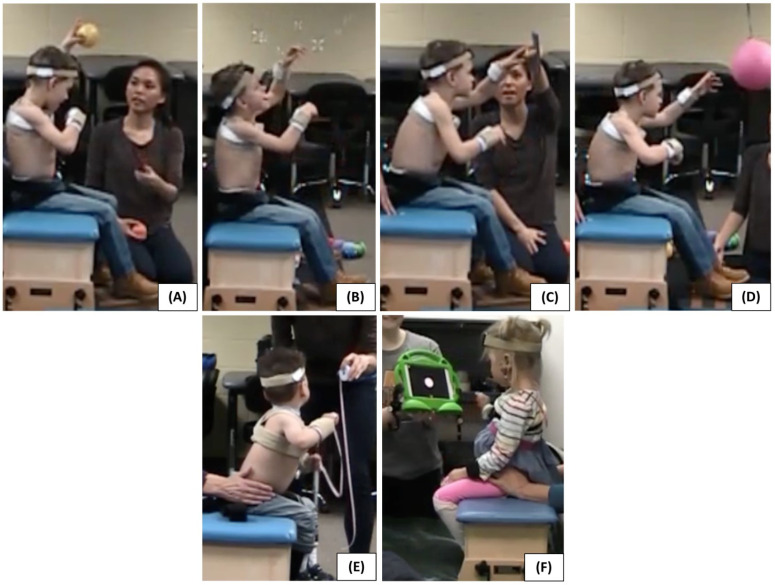
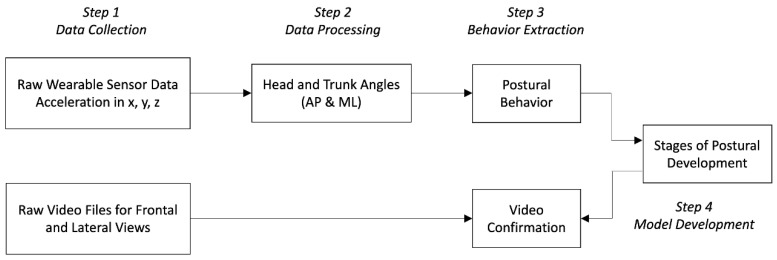
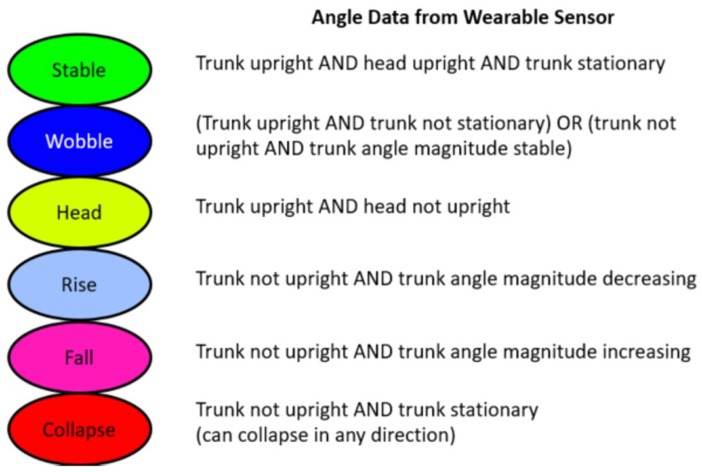
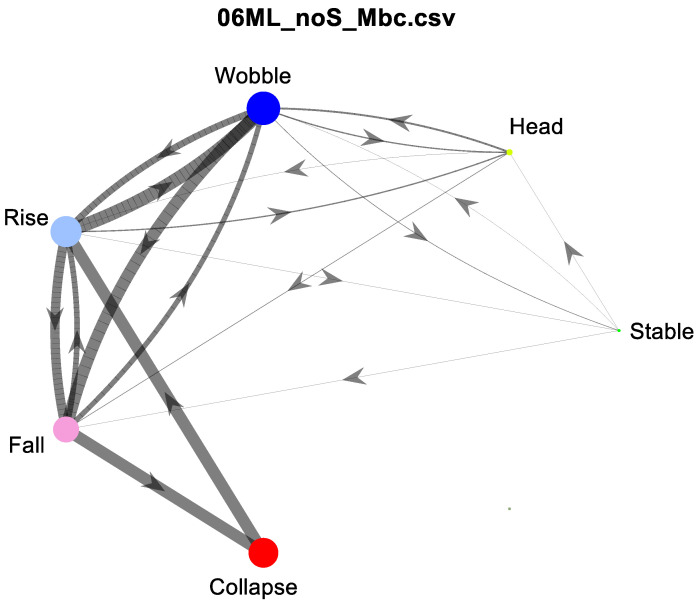
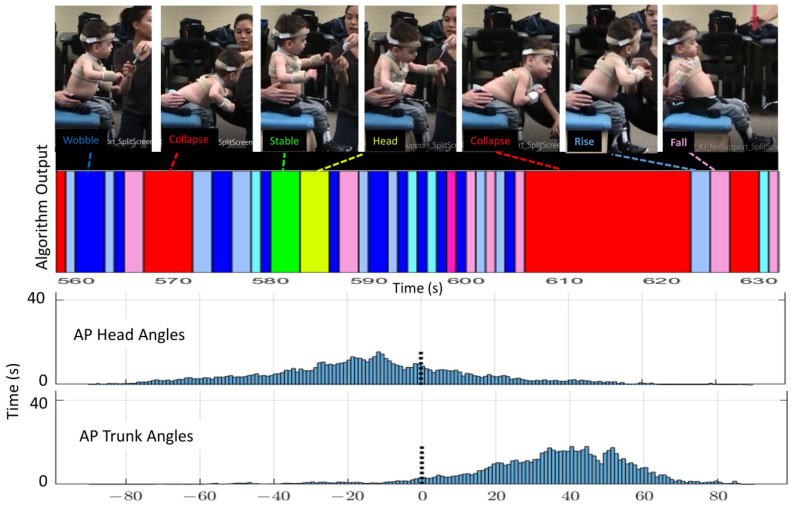
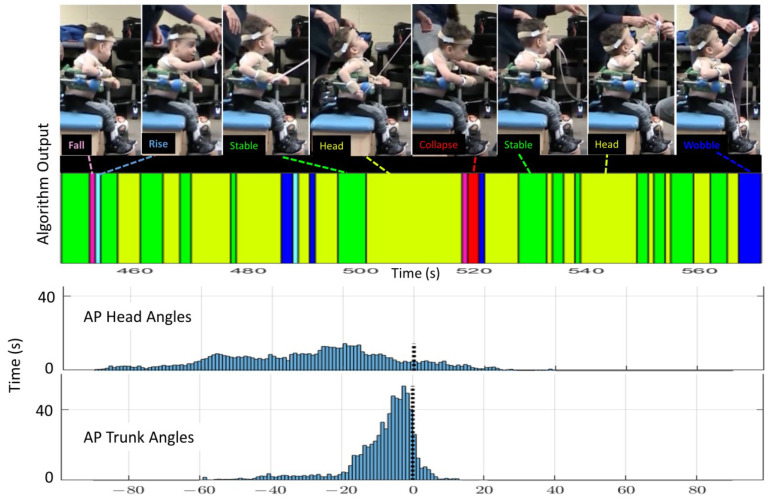
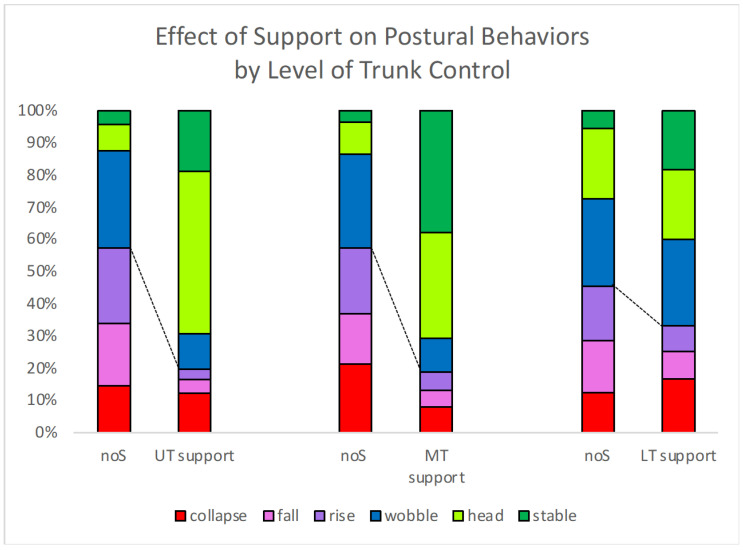
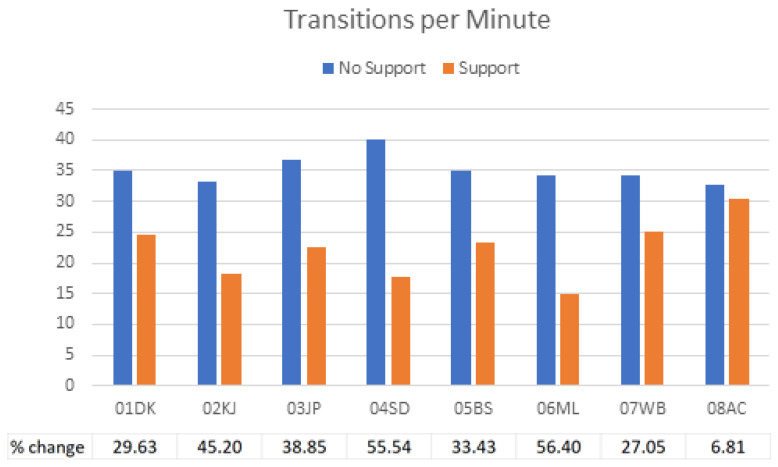
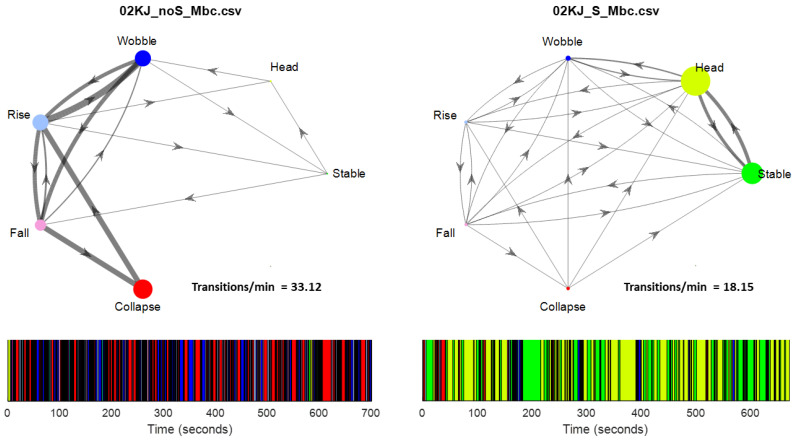
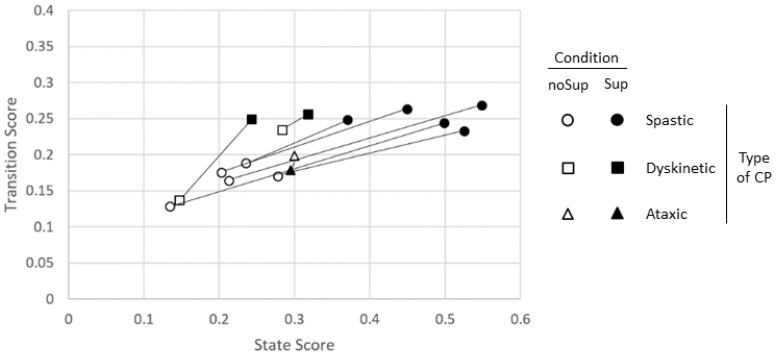
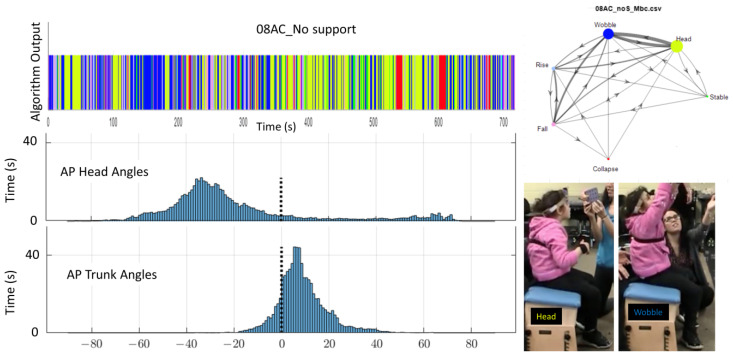
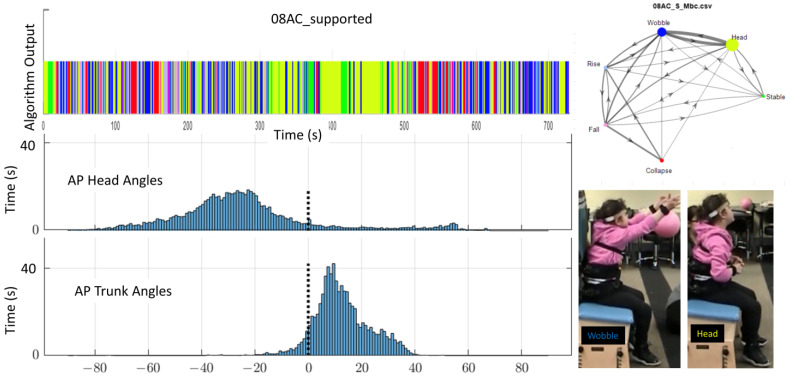
Objective, quantitative postural data is limited for individuals who are non-ambulatory, especially for those who have not yet developed trunk control for sitting. There are no gold standard measurements to monitor the emergence of upright trunk control. Quantification of intermediate levels of postural control is critically needed to improve research and intervention for these individuals. Accelerometers and video were used to record postural alignment and stability for eight children with severe cerebral palsy aged 2 to 13 years, under two conditions, seated on a bench with only pelvic support and with additional thoracic support. This study developed an algorithm to classify vertical alignment and states of upright control; Stable, Wobble, Collapse, Rise and Fall from accelerometer data. Next, a Markov chain model was created to calculate a normative score for postural state and transition for each participant with each level of support. This tool allowed quantification of behaviors previously not captured in adult-based postural sway measures. Histogram and video recordings were used to confirm the output of the algorithm. Together, this tool revealed that providing external support allowed all participants: (1) to increase their time spent in the Stable state, and (2) to reduce the frequency of transitions between states. Furthermore, all participants except one showed improved state and transition scores when given external support.
Keywords: accelerometer; assessment; biomechanical algorithm; cerebral palsy; motor control; postural development model; trunk.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Changes in trunk sway and impairment during sitting and standing in children with cerebral palsy.Technol Health Care. 2018;26(5):761-768. doi: 10.3233/THC-181301. Technol Health Care. 2018. PMID: 29991150
-
Impact of dual task on postural sway during sit-to-stand movement in children with unilateral cerebral palsy.Clin Biomech (Bristol). 2020 Aug;78:105072. doi: 10.1016/j.clinbiomech.2020.105072. Epub 2020 Jun 3. Clin Biomech (Bristol). 2020. PMID: 32562882
-
Effects of Visual Manipulation in Sit-to-Stand Movement in Children With Cerebral Palsy.J Mot Behav. 2018 Sep-Oct;50(5):486-491. doi: 10.1080/00222895.2017.1367641. Epub 2017 Oct 4. J Mot Behav. 2018. PMID: 28976286
-
Use of accelerometry to investigate standing and dynamic body balance in people with cerebral palsy: A systematic review.Gait Posture. 2022 Jul;96:357-364. doi: 10.1016/j.gaitpost.2022.06.017. Epub 2022 Jul 7. Gait Posture. 2022. PMID: 35820240
-
The effect of trunk muscle fatigue on postural control of upright stance: A systematic review.Gait Posture. 2019 Jul;72:167-174. doi: 10.1016/j.gaitpost.2019.06.010. Epub 2019 Jun 11. Gait Posture. 2019. PMID: 31207565
References
-
- Soo B., Howard J.J., Boyd R.N., Reid S.M., Lanigan A., Wolfe R., Graham H.K. Hip displacement in cerebral palsy. J. Bone Jt. Surg. 2006;88A:121–129. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
