

This is a preprint.
Symptom-led staging for primary progressive aphasia
- PMID: 36993460
- PMCID: PMC10055437
- DOI: 10.1101/2023.03.13.23286972
Symptom-led staging for primary progressive aphasia
Update in
-
Symptom-led staging for semantic and non-fluent/agrammatic variants of primary progressive aphasia.Alzheimers Dement. 2024 Jan;20(1):195-210. doi: 10.1002/alz.13415. Epub 2023 Aug 7. Alzheimers Dement. 2024. PMID: 37548125 Free PMC article.
Abstract
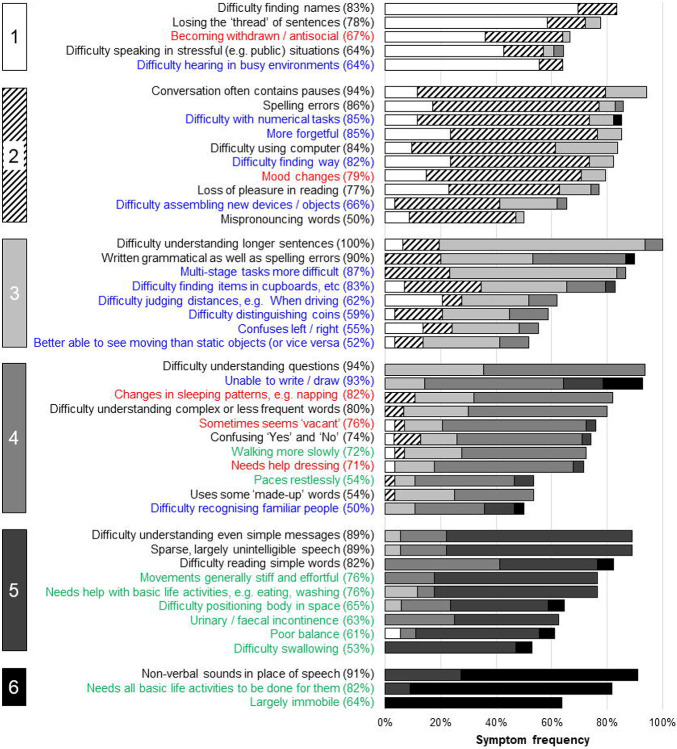
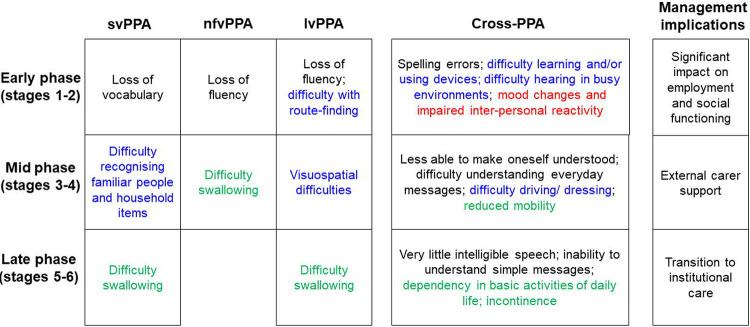
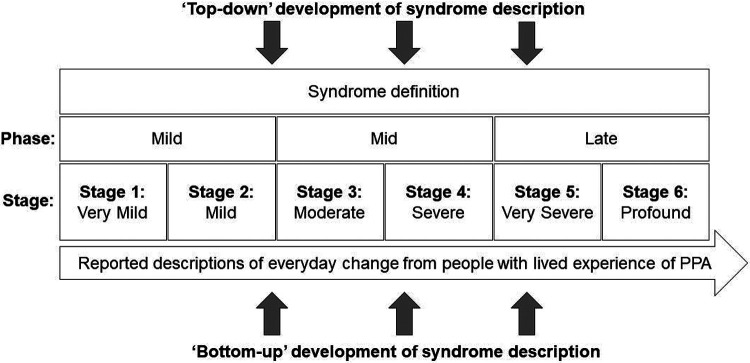
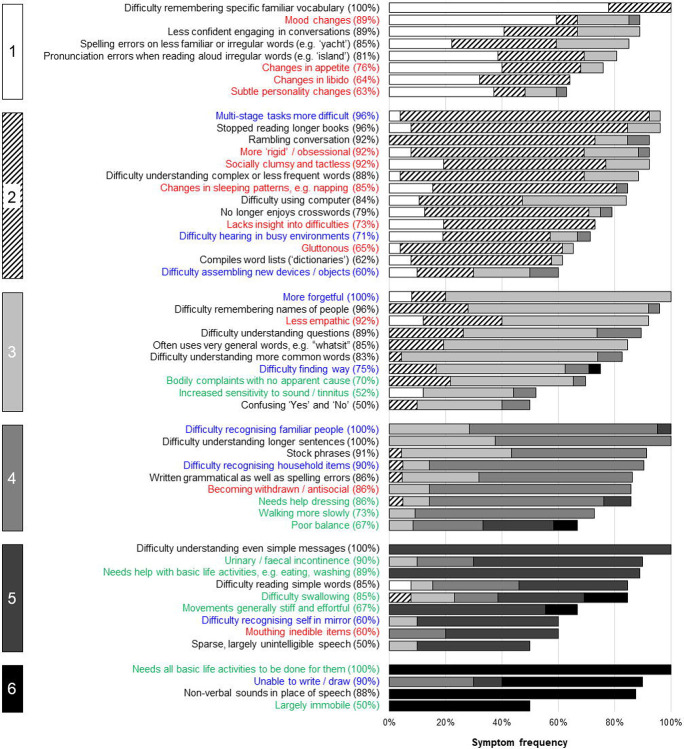
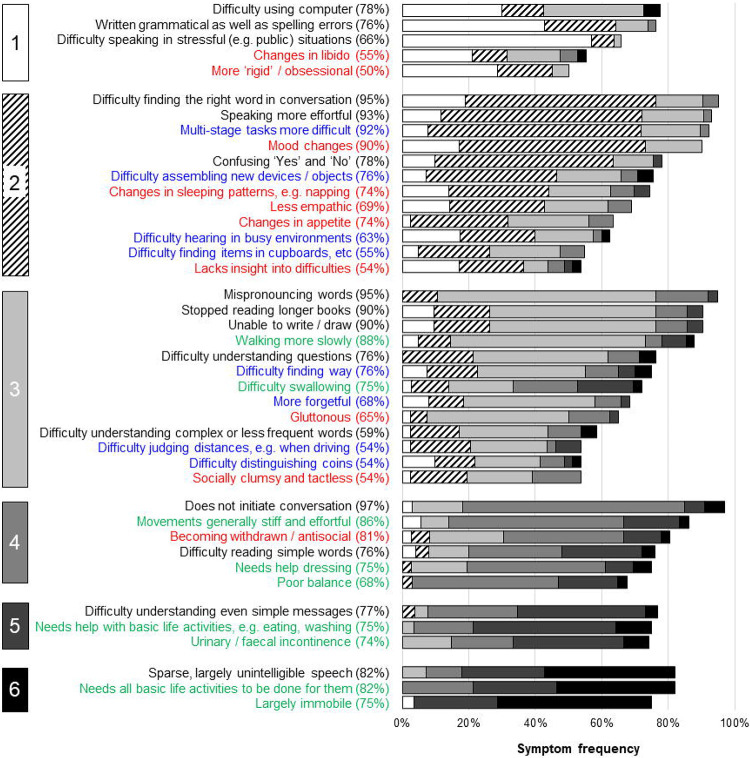
The primary progressive aphasias (PPA) present complex and diverse challenges of diagnosis, management and prognosis. A clinically-informed, syndromic staging system for PPA would take a substantial step toward meeting these challenges. This study addressed this need using detailed, multi-domain mixed-methods symptom surveys of people with lived experience in a large international PPA cohort. We administered structured online surveys to caregivers of patients with a canonical PPA syndromic variant (nonfluent/agrammatic (nvPPA), semantic (svPPA) or logopenic (lvPPA)). In an 'exploratory' survey, a putative list and ordering of verbal communication and nonverbal functioning (nonverbal thinking, conduct and wellbeing, physical) symptoms was administered to 118 caregiver members of the UK national PPA Support Group. Based on feedback, we expanded the symptom list and created six provisional clinical stages for each PPA subtype. In a 'consolidation' survey, these stages were presented to 110 caregiver members of UK and Australian PPA Support Groups, and refined based on quantitative and qualitative feedback. Symptoms were retained if rated as 'present' by a majority (at least 50%) of respondents representing that PPA syndrome, and assigned to a consolidated stage based on majority consensus; the confidence of assignment was estimated for each symptom as the proportion of respondents in agreement with the final staging for that symptom. Qualitative responses were analysed using framework analysis. For each PPA syndrome, six stages ranging from 1 ('Very mild') to 6 ('Profound') were identified; earliest stages were distinguished by syndromic hallmark symptoms of communication dysfunction, with increasing trans-syndromic convergence and dependency for basic activities of daily living at later stages. Spelling errors, hearing changes and nonverbal behavioural features were reported at early stages in all syndromes. As the illness evolved, swallowing and mobility problems were reported earlier in nfvPPA than other syndromes, while difficulty recognising familiar people and household items characterised svPPA and visuospatial symptoms were more prominent in lvPPA. Overall confidence of symptom staging was higher for svPPA than other syndromes. Across syndromes, functional milestones were identified as key deficits that predict the sequence of major daily life impacts and associated management needs. Qualitatively, we identified five major themes encompassing 15 subthemes capturing respondents' experiences of PPA and suggestions for staging implementation. This work introduces a prototypical, symptom-led staging scheme for canonical PPA syndromes: the PPA Progression Planning Aid (PPA 2 ). Our findings have implications for diagnostic and care pathway guidelines, trial design and personalised prognosis and treatment for people living with these diseases.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials