

This is a preprint.
CDH1 loss promotes diffuse-type gastric cancer tumorigenesis via epigenetic reprogramming and immune evasion
- PMID: 36993615
- PMCID: PMC10055394
- DOI: 10.1101/2023.03.23.533976
CDH1 loss promotes diffuse-type gastric cancer tumorigenesis via epigenetic reprogramming and immune evasion
Update in
-
E-cadherin loss drives diffuse-type gastric tumorigenesis via EZH2-mediated reprogramming.J Exp Med. 2024 Apr 1;221(4):e20230561. doi: 10.1084/jem.20230561. Epub 2024 Feb 27. J Exp Med. 2024. PMID: 38411616 Free PMC article.
Abstract
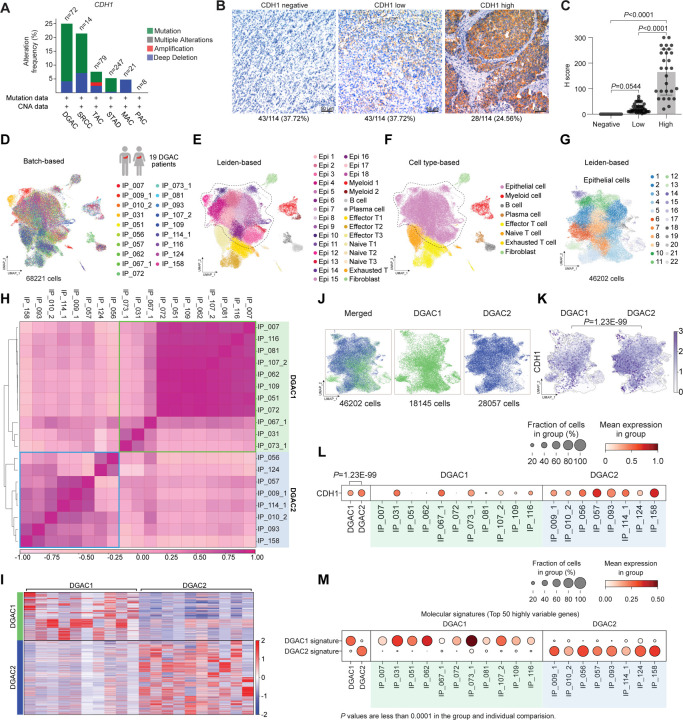
Diffuse-type gastric adenocarcinoma (DGAC) is a deadly cancer often diagnosed late and resistant to treatment. While hereditary DGAC is linked to CDH1 gene mutations, causing E-Cadherin loss, its role in sporadic DGAC is unclear. We discovered CDH1 inactivation in a subset of DGAC patient tumors. Analyzing single-cell transcriptomes in malignant ascites, we identified two DGAC subtypes: DGAC1 (CDH1 loss) and DGAC2 (lacking immune response). DGAC1 displayed distinct molecular signatures, activated DGAC-related pathways, and an abundance of exhausted T cells in ascites. Genetically engineered murine gastric organoids showed that Cdh1 knock-out (KO), KrasG12D, Trp53 KO (EKP) accelerates tumorigenesis with immune evasion compared to KrasG12D, Trp53 KO (KP). We also identified EZH2 as a key mediator promoting CDH1 loss-associated DGAC tumorigenesis. These findings highlight DGAC's molecular diversity and potential for personalized treatment in CDH1-inactivated patients.
Keywords: CDH1; E-Cadherin; EZH2; cancer subtyping; diffuse-type gastric adenocarcinoma; gastric cancer; gastric organoids; immune evasion; immune landscape remodeling; single-cell transcriptomics.
Figures




References
-
- Aibar S., Gonzalez-Blas C. B., Moerman T., Huynh-Thu V. A., Imrichova H., Hulselmans G., Rambow F., Marine J. C., Geurts P., Aerts J., van den Oord J., Atak Z. K., Wouters J. and Aerts S.. 2017. SCENIC: single-cell regulatory network inference and clustering. Nat Methods 14: 1083–1086. - PMC - PubMed
-
- Ajani J. A., D’Amico T. A., Bentrem D. J., Chao J., Cooke D., Corvera C., Das P., Enzinger P. C., Enzler T., Fanta P., Farjah F., Gerdes H., Gibson M. K., Hochwald S., Hofstetter W. L., Ilson D. H., Keswani R. N., Kim S., Kleinberg L. R., Klempner S. J., Lacy J., Ly Q. P., Matkowskyj K. A., McNamara M., Mulcahy M. F., Outlaw D., Park H., Perry K. A., Pimiento J., Poultsides G. A., Reznik S., Roses R. E., Strong V. E., Su S., Wang H. L., Wiesner G., Willett C. G., Yakoub D., Yoon H., McMillian N. and Pluchino L. A.. 2022. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 20: 167–192. - PubMed
-
- Al-Ahmadie H. A., Iyer G., Lee B. H., Scott S. N., Mehra R., Bagrodia A., Jordan E. J., Gao S. P., Ramirez R., Cha E. K., Desai N. B., Zabor E. C., Ostrovnaya I., Gopalan A., Chen Y. B., Fine S. W., Tickoo S. K., Gandhi A., Hreiki J., Viale A., Arcila M. E., Dalbagni G., Rosenberg J. E., Bochner B. H., Bajorin D. F., Berger M. F., Reuter V. E., Taylor B. S. and Solit D. B.. 2016. Frequent somatic CDH1 loss-of-function mutations in plasmacytoid variant bladder cancer. Nat Genet 48: 356–358. - PMC - PubMed
-
- Ashburner M., Ball C. A., Blake J. A., Botstein D., Butler H., Cherry J. M., Davis A. P., Dolinski K., Dwight S. S., Eppig J. T., Harris M. A., Hill D. P., Issel-Tarver L., Kasarskis A., Lewis S., Matese J. C., Richardson J. E., Ringwald M., Rubin G. M. and Sherlock G.. 2000. Gene ontology: tool for the unification of biology. The Gene Ontology Consortium. Nat Genet 25: 25–29. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous