

Prolonged PR interval and incidence of atrial fibrillation, heart failure admissions, and mortality in patients with implanted cardiac devices: A real-world survey
- PMID: 36993911
- PMCID: PMC10041089
- DOI: 10.1016/j.hroo.2022.12.009
Prolonged PR interval and incidence of atrial fibrillation, heart failure admissions, and mortality in patients with implanted cardiac devices: A real-world survey
Abstract
Background: Prolongation of the PR interval has long been considered a benign condition, particularly in the setting of nonstructural heart disease.
Objective: The purpose of this study was to investigate the effect of PR interval on various well-adjudicated cardiovascular outcomes using a large real-world population data of patients with implanted dual-chamber permanent pacemakers or implantable cardioverter-defibrillators.
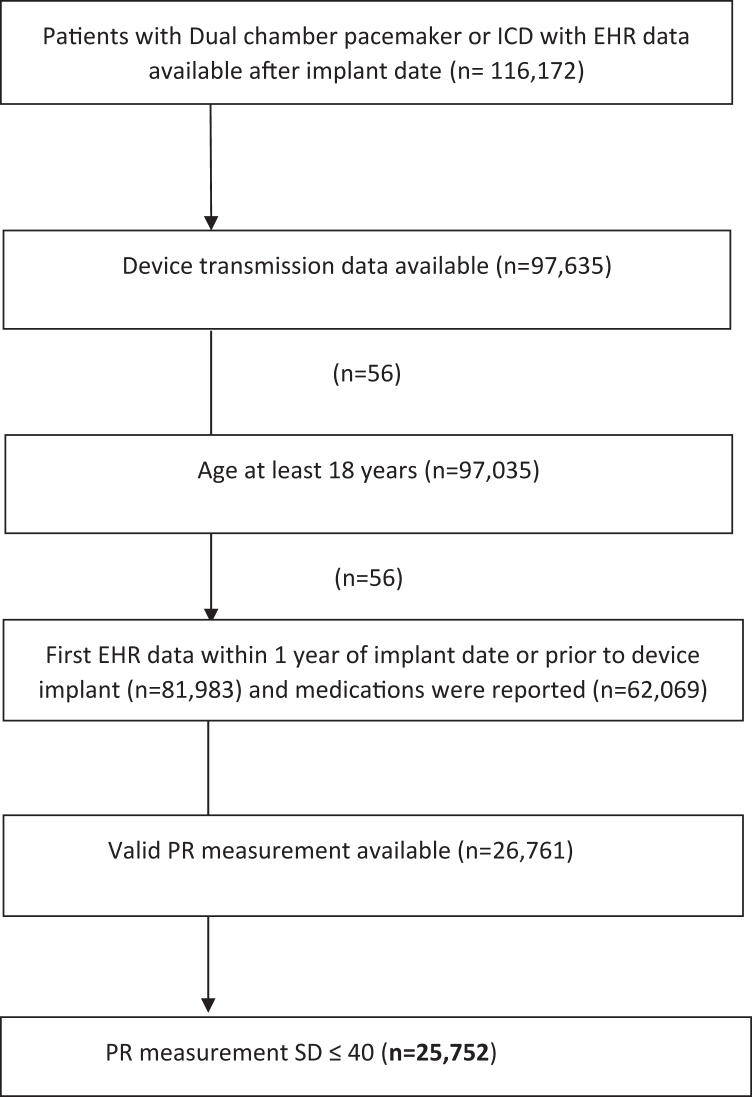
Methods: PR intervals were measured during remote transmissions in patients with implanted permanent pacemakers or implantable cardioverter-defibrillators. Study endpoints (time to the first occurrence of AF, heart failure hospitalization [HFH], or death) were obtained between January 2007 and June 2019 from the deidentified Optum de-identified Electronic Health Record dataset.
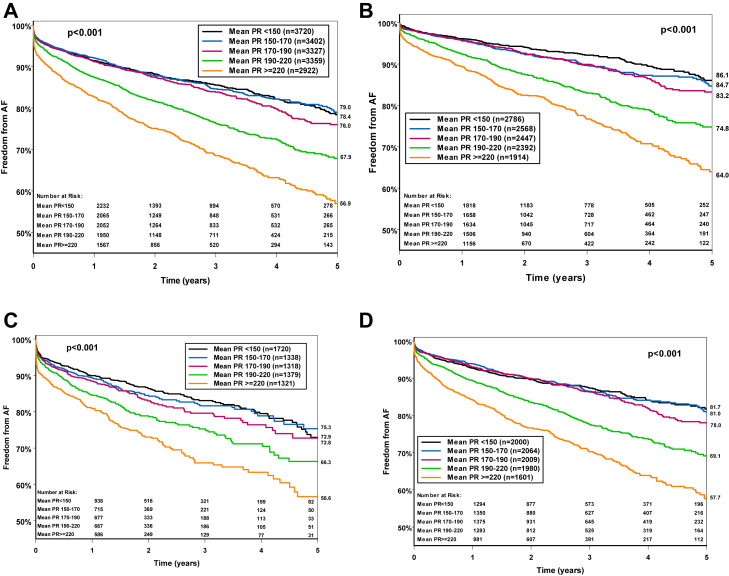
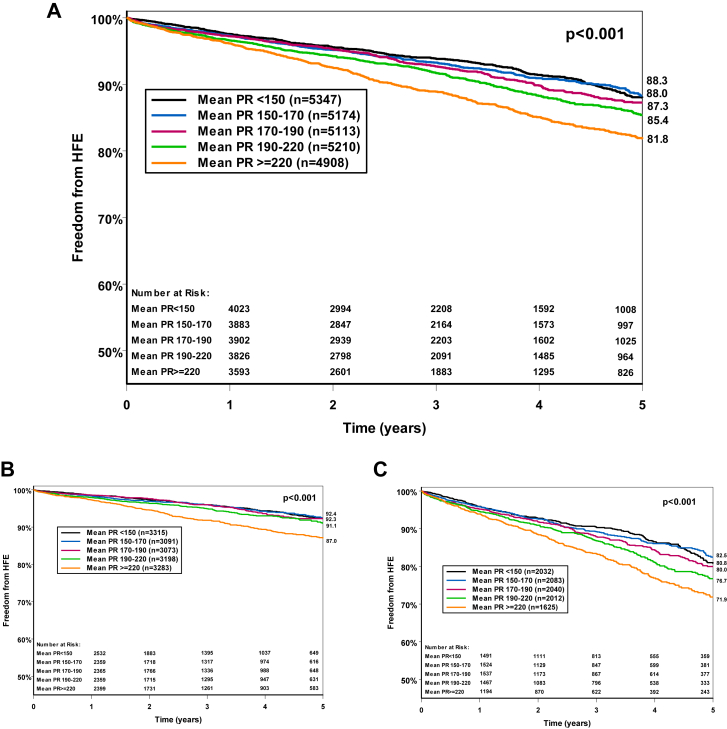
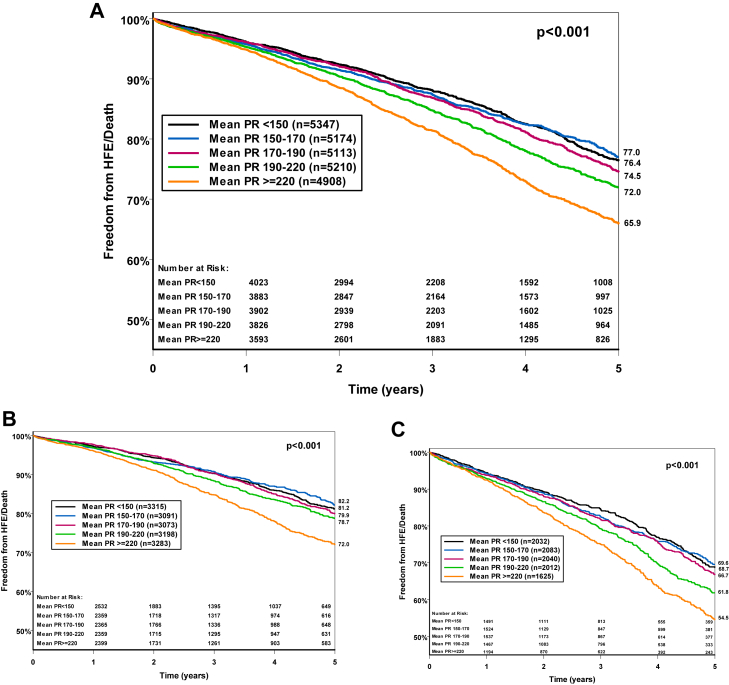
Results: A total of 25,752 patients (age 69.3 ± 13.9 years; 58% male) were evaluated. The average intrinsic PR interval was 185 ± 55 ms. In the subset of 16,730 patients with available long-term device diagnostic data, a total of 2555 (15.3%) individuals developed AF during 2.59 ± 2.18 years of follow-up. The incidence of AF was significantly higher (up to 30%) in patients with a longer PR interval (ie, PR interval ≥270 ms; P < .05). Time-to-event survival analysis and multivariable analysis showed that PR interval ≥190 ms was significantly associated with higher incidence of AF, HFH, or HFH or death when compared with shorter PR intervals (P < .05 for all 3 parameters).
Conclusion: In a large real-world population of patients with implanted devices, PR interval prolongation was significantly associated with increased incidence of AF, HFH, or death.
Keywords: Atrial fibrillation; Clinical outcomes; Heart failure; PR interval; Pacemaker.
© 2022 Heart Rhythm Society. Published by Elsevier Inc.
Figures
Similar articles
-
Association between ventricular pacing and persistent atrial fibrillation in patients indicated to elective pacemaker replacement: Results of the Prefer for Elective Replacement MVP (PreFER MVP) randomized study.Heart Rhythm. 2015 Nov;12(11):2239-46. doi: 10.1016/j.hrthm.2015.06.041. Epub 2015 Jun 30. Heart Rhythm. 2015. PMID: 26142300 Clinical Trial.
-
Stratifying patients at the risk of heart failure hospitalization using existing device diagnostic thresholds.Heart Lung. 2015 Mar-Apr;44(2):129-36. doi: 10.1016/j.hrtlng.2014.07.007. Epub 2014 Dec 24. Heart Lung. 2015. PMID: 25543319 Free PMC article.
-
Occurrence of significant long PR intervals in patients implanted for sinus node dysfunction and monitored with SafeR™: The PRECISE study.Arch Cardiovasc Dis. 2019 Mar;112(3):153-161. doi: 10.1016/j.acvd.2018.09.005. Epub 2018 Dec 26. Arch Cardiovasc Dis. 2019. PMID: 30594571
-
Remote Monitoring of Implantable Cardioverter-Defibrillators, Cardiac Resynchronization Therapy and Permanent Pacemakers: A Health Technology Assessment.Ont Health Technol Assess Ser. 2018 Oct 24;18(7):1-199. eCollection 2018. Ont Health Technol Assess Ser. 2018. PMID: 30443279 Free PMC article. Review.
-
Association between atrial fibrillation and patient-important outcomes in heart failure patients with implantable cardioverter-defibrillators: a systematic review and meta-analysis.Eur Heart J Qual Care Clin Outcomes. 2019 Apr 1;5(2):96-104. doi: 10.1093/ehjqcco/qcy054. Eur Heart J Qual Care Clin Outcomes. 2019. PMID: 30462233
Cited by
-
Association of same-day urinary phenol levels and cardiac electrical alterations: analysis of the Fernald Community Cohort.Environ Health. 2024 Sep 19;23(1):76. doi: 10.1186/s12940-024-01114-x. Environ Health. 2024. PMID: 39300535 Free PMC article.
-
Association of same-day urinary phenol levels and cardiac electrical alterations: analysis of the Fernald Community Cohort.Res Sq [Preprint]. 2024 May 31:rs.3.rs-4445657. doi: 10.21203/rs.3.rs-4445657/v1. Res Sq. 2024. Update in: Environ Health. 2024 Sep 19;23(1):76. doi: 10.1186/s12940-024-01114-x. PMID: 38853936 Free PMC article. Updated. Preprint.
-
Association of electrocardiogram features with risk of obstructed sleep apnea: a population-based cohort study.Sleep Breath. 2025 Feb 11;29(1):96. doi: 10.1007/s11325-025-03266-7. Sleep Breath. 2025. PMID: 39934598
-
Vascular function assessed by flow-mediated vasodilation and nitroglycerine-induced vasodilation in subjects with first-degree atrioventricular block.Sci Rep. 2024 Dec 5;14(1):30315. doi: 10.1038/s41598-024-81211-6. Sci Rep. 2024. PMID: 39638866 Free PMC article.
-
Can prolonged P-R interval predict clinical outcomes in non-ST elevation acute coronary syndrome patients?BMC Cardiovasc Disord. 2024 Mar 2;24(1):137. doi: 10.1186/s12872-024-03809-y. BMC Cardiovasc Disord. 2024. PMID: 38431589 Free PMC article.
References
-
- Braunwald E., Mann D.L., Zipes D.P. 11th ed. Elsevier Saunders; Philadelphia, PA: 2019. Braunwald's heart disease.
-
- Perlman L.V., Ostrander L.D., Keller J.B., Chiang B.N. An epidemiologic study of first degree atrioventricular block in Tecumseh, Michigan. Chest. 1971;59:40–46. - PubMed
-
- Kwok C.S., Rashid M., Beynon R., et al. Prolonged PR interval, first-degree heart block and adverse cardiovascular outcomes: a systematic review and meta-analysis. Heart. 2016;102:672–680. - PubMed
-
- Mymin D., Mathewson F.A., Tate R.B., Manfreda J. The natural history of primary first-degree atrioventricular heart block. N Engl J Med. 1986;315:1183–1187. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
