

Aldosterone: Renal Action and Physiological Effects
- PMID: 36994769
- PMCID: PMC11472823
- DOI: 10.1002/cphy.c190043
Aldosterone: Renal Action and Physiological Effects
Abstract
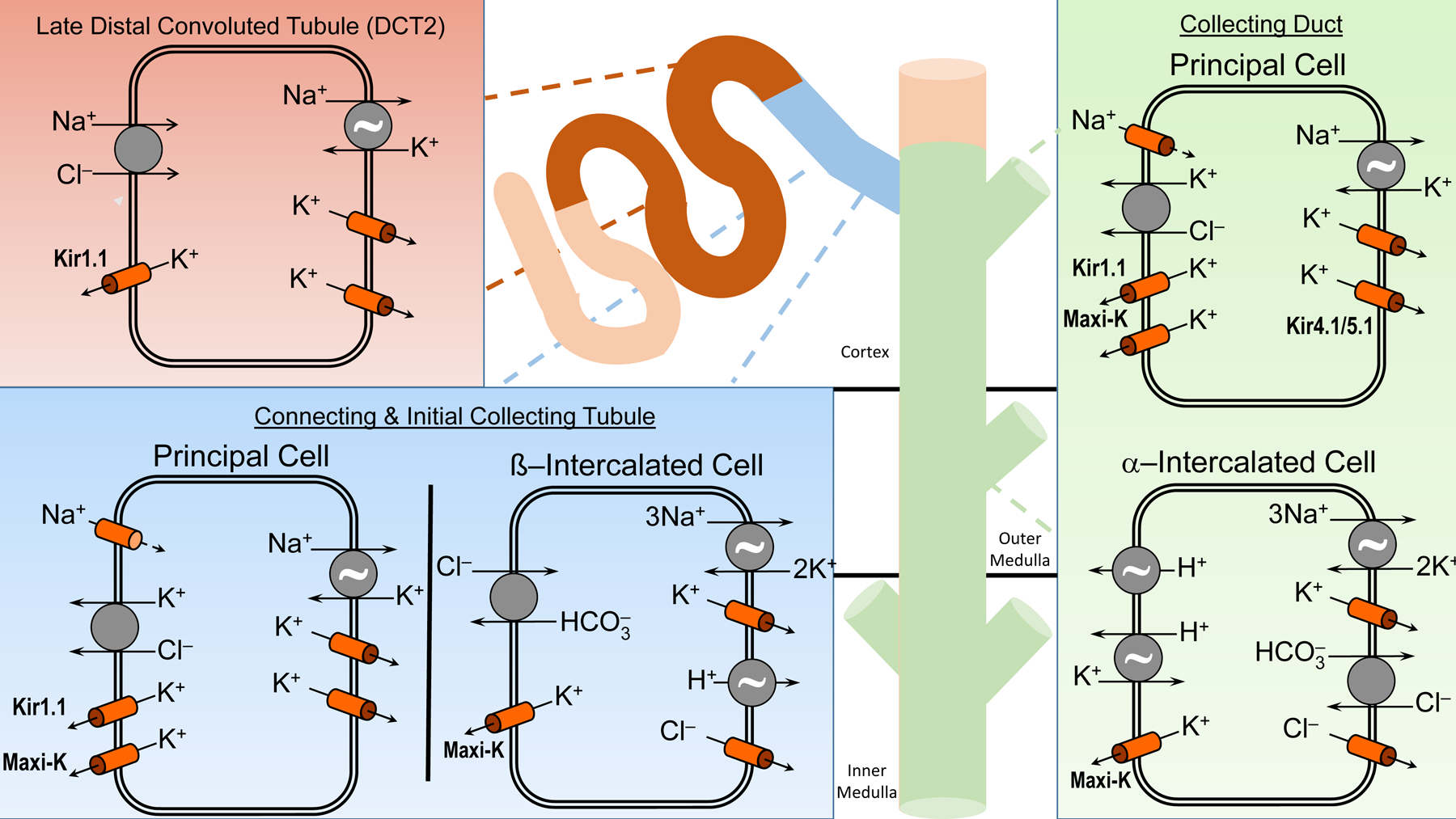
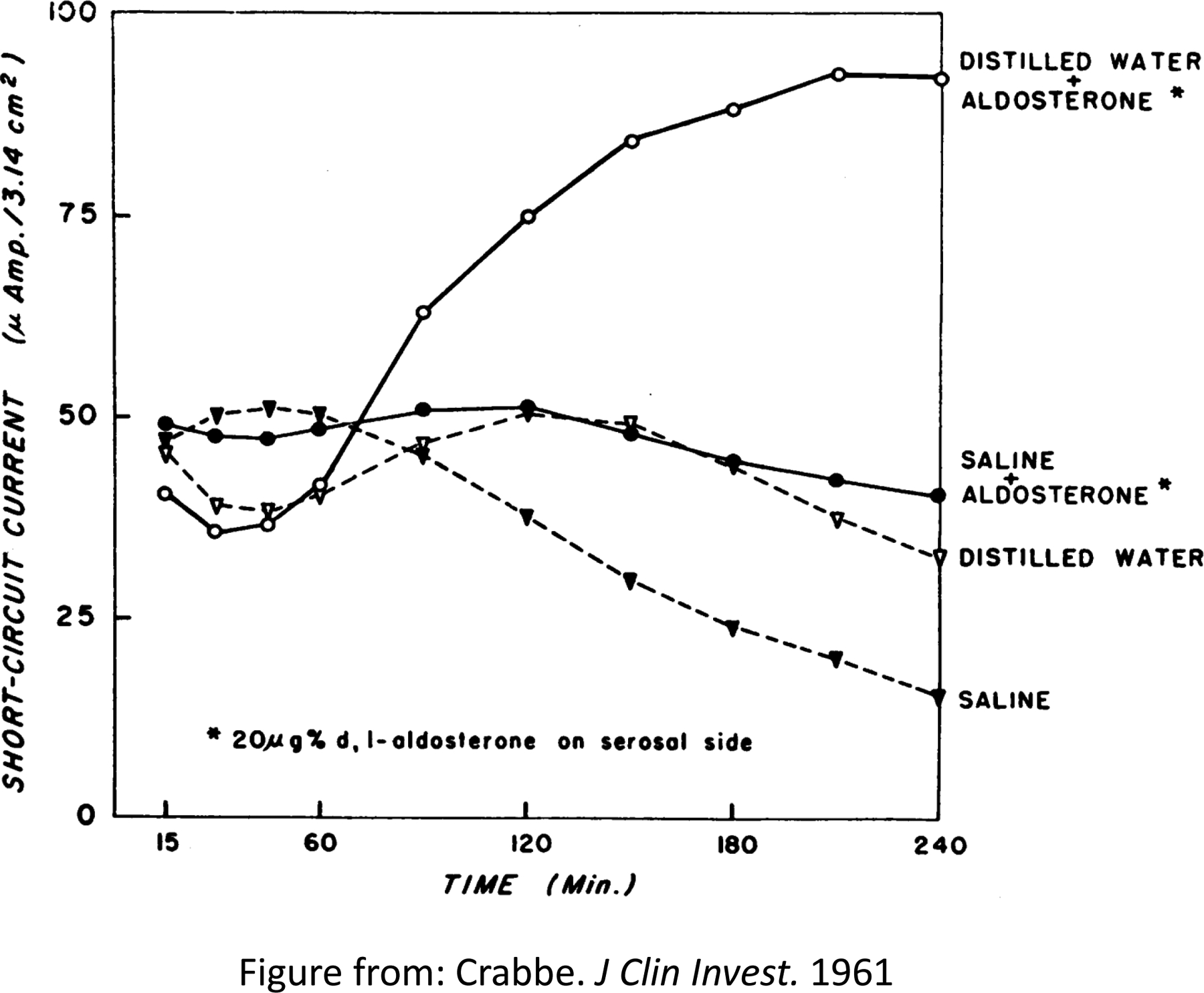
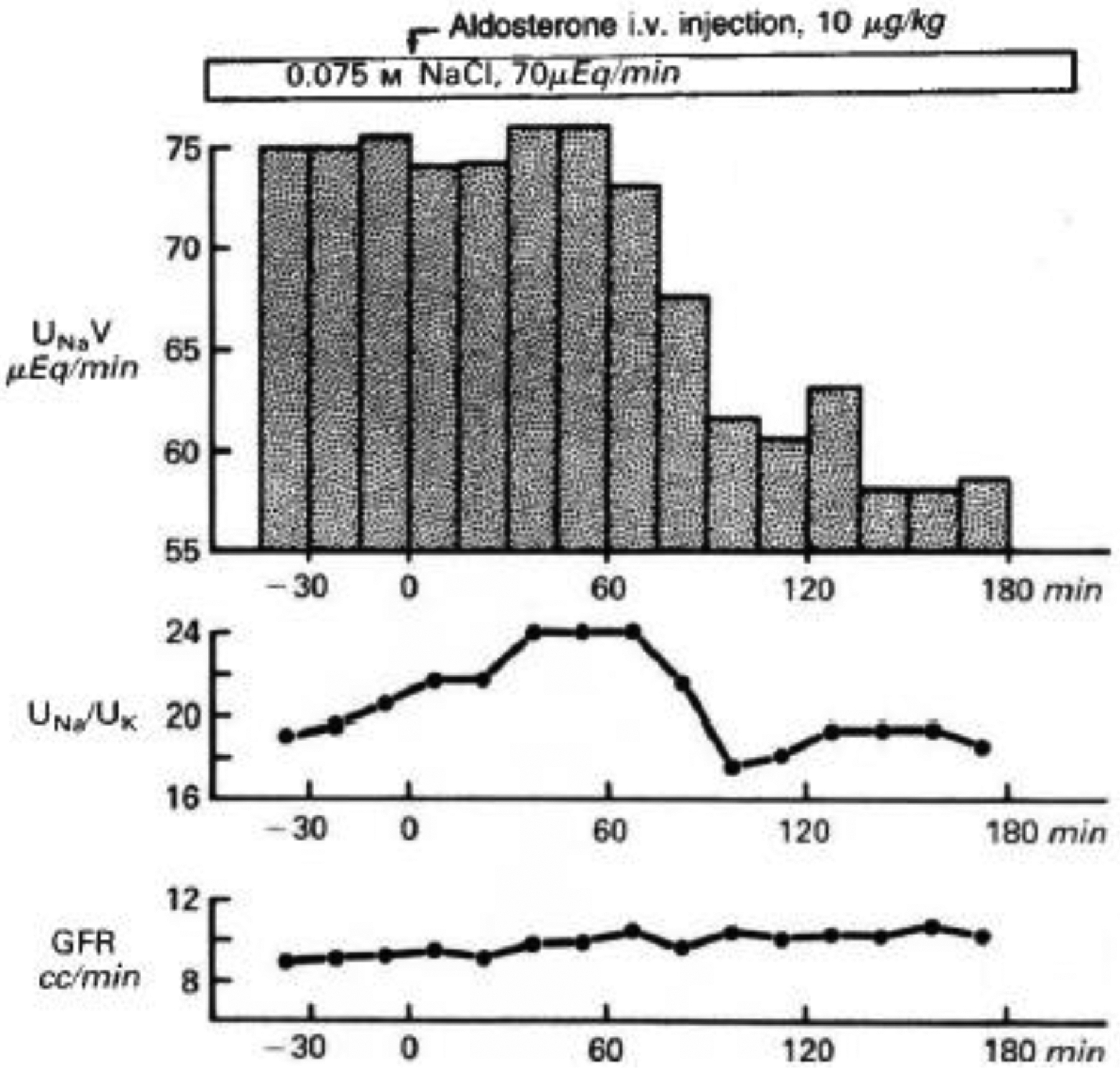
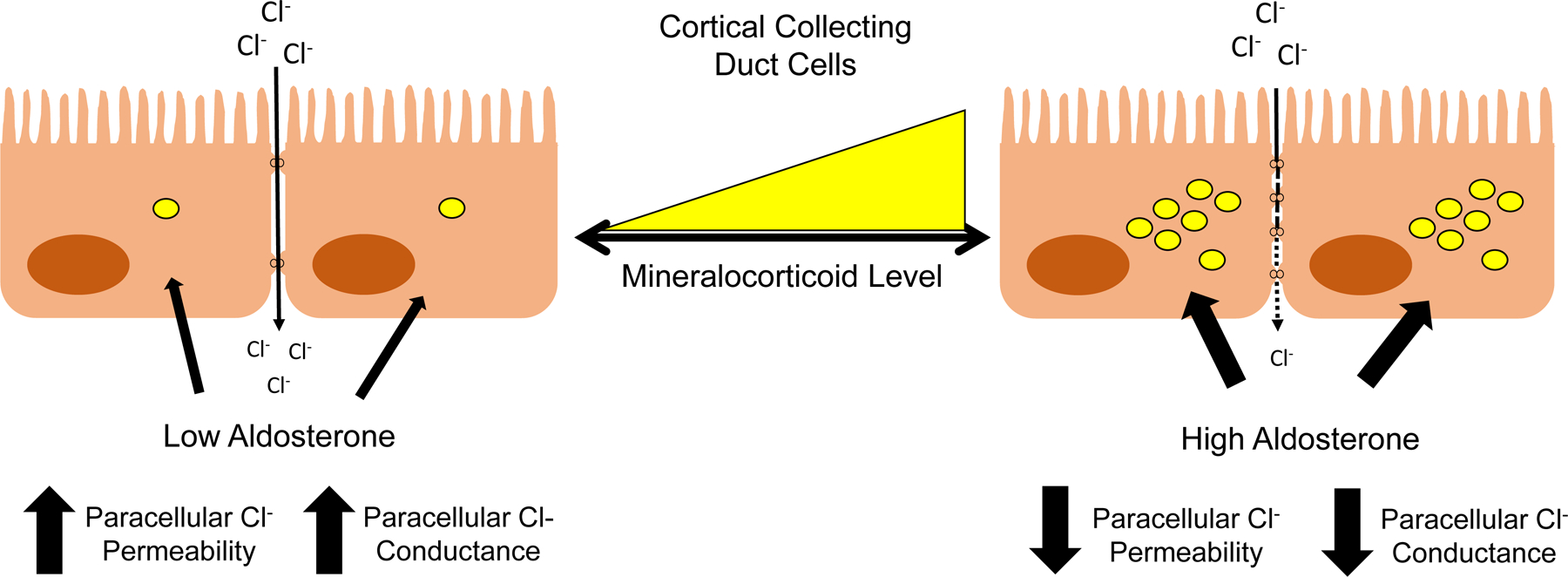
Aldosterone exerts profound effects on renal and cardiovascular physiology. In the kidney, aldosterone acts to preserve electrolyte and acid-base balance in response to changes in dietary sodium (Na+ ) or potassium (K+ ) intake. These physiological actions, principally through activation of mineralocorticoid receptors (MRs), have important effects particularly in patients with renal and cardiovascular disease as demonstrated by multiple clinical trials. Multiple factors, be they genetic, humoral, dietary, or otherwise, can play a role in influencing the rate of aldosterone synthesis and secretion from the adrenal cortex. Normally, aldosterone secretion and action respond to dietary Na+ intake. In the kidney, the distal nephron and collecting duct are the main targets of aldosterone and MR action, which stimulates Na+ absorption in part via the epithelial Na+ channel (ENaC), the principal channel responsible for the fine-tuning of Na+ balance. Our understanding of the regulatory factors that allow aldosterone, via multiple signaling pathways, to function properly clearly implicates this hormone as central to many pathophysiological effects that become dysfunctional in disease states. Numerous pathologies that affect blood pressure (BP), electrolyte balance, and overall cardiovascular health are due to abnormal secretion of aldosterone, mutations in MR, ENaC, or effectors and modulators of their action. Study of the mechanisms of these pathologies has allowed researchers and clinicians to create novel dietary and pharmacological targets to improve human health. This article covers the regulation of aldosterone synthesis and secretion, receptors, effector molecules, and signaling pathways that modulate its action in the kidney. We also consider the role of aldosterone in disease and the benefit of mineralocorticoid antagonists. © 2023 American Physiological Society. Compr Physiol 13:4409-4491, 2023.
This article is a U.S. Government work and is in the public domain in the U.S.A.
Figures
References
-
- Ackermann D, Gresko N, Carrel M, Loffing-Cueni D, Habermehl D, Gomez-Sanchez C, Rossier BC, and Loffing J. In vivo nuclear translocation of mineralocorticoid and glucocorticoid receptors in rat kidney: differential effect of corticosteroids along the distal tubule. Am J Physiol Renal Physiol 299: F1473–1485, 2010. - PubMed
-
- Agarwal AK, Mune T, Monder C, and White PC. NAD(+)-dependent isoform of 11 beta-hydroxysteroid dehydrogenase. Cloning and characterization of cDNA from sheep kidney. J Biol Chem 269: 25959–25962, 1994. - PubMed
-
- Agrawal S, He JC, and Tharaux PL. Nuclear receptors in podocyte biology and glomerular disease. Nat Rev Nephrol 17: 185–204, 2021. - PubMed
-
- Aguilera G, and Catt KJ. Participation of voltage-dependent calcium channels in the regulation of adrenal glomerulosa function by angiotensin II and potassium. Endocrinology 118: 112–118, 1986. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
