

Extended Analysis of HIV Infection in Cisgender Men and Transgender Women Who Have Sex with Men Receiving Injectable Cabotegravir for HIV Prevention: HPTN 083
- PMID: 36995219
- PMCID: PMC10112247
- DOI: 10.1128/aac.00053-23
Extended Analysis of HIV Infection in Cisgender Men and Transgender Women Who Have Sex with Men Receiving Injectable Cabotegravir for HIV Prevention: HPTN 083
Abstract
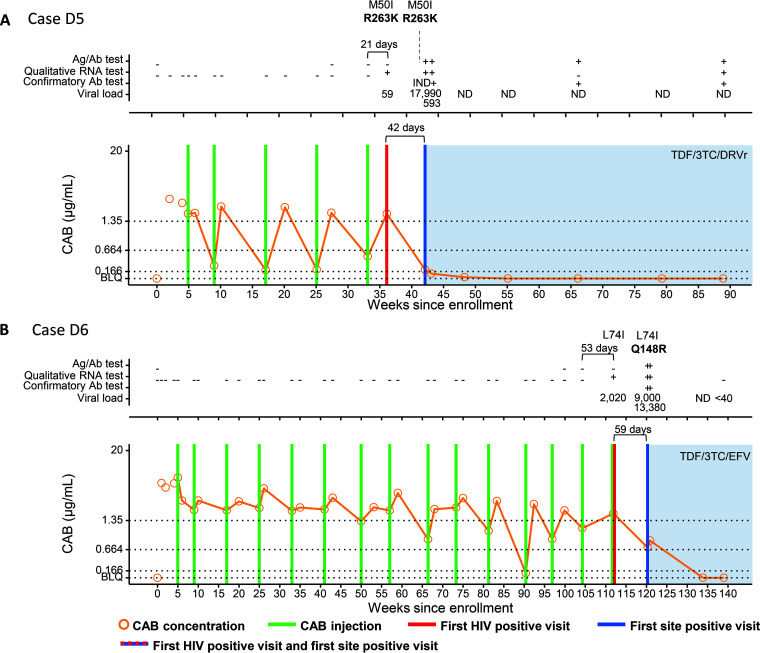
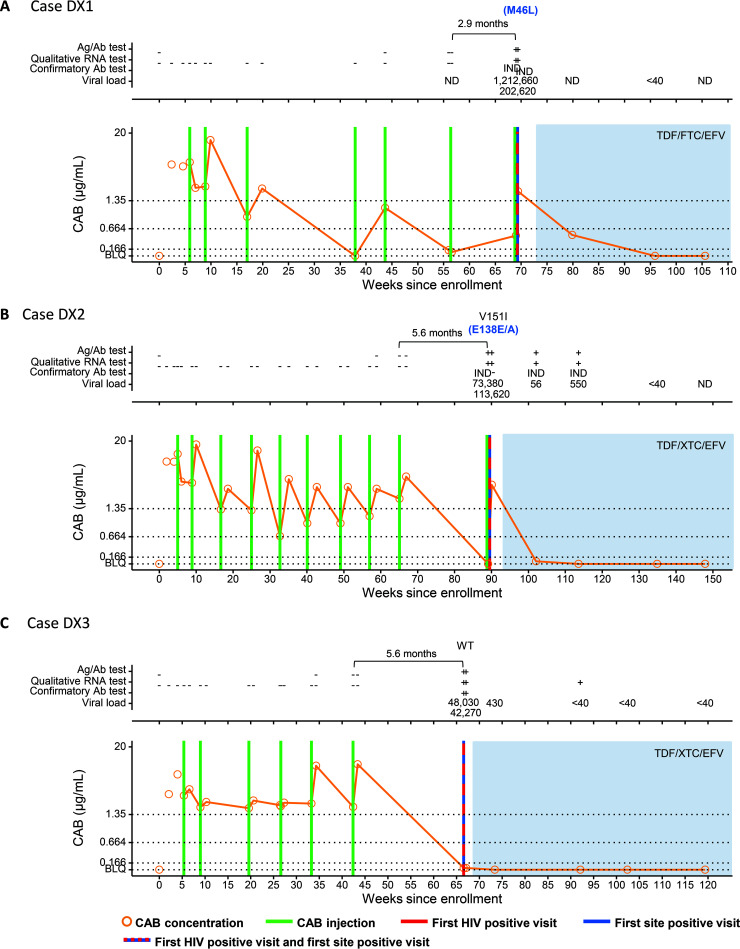
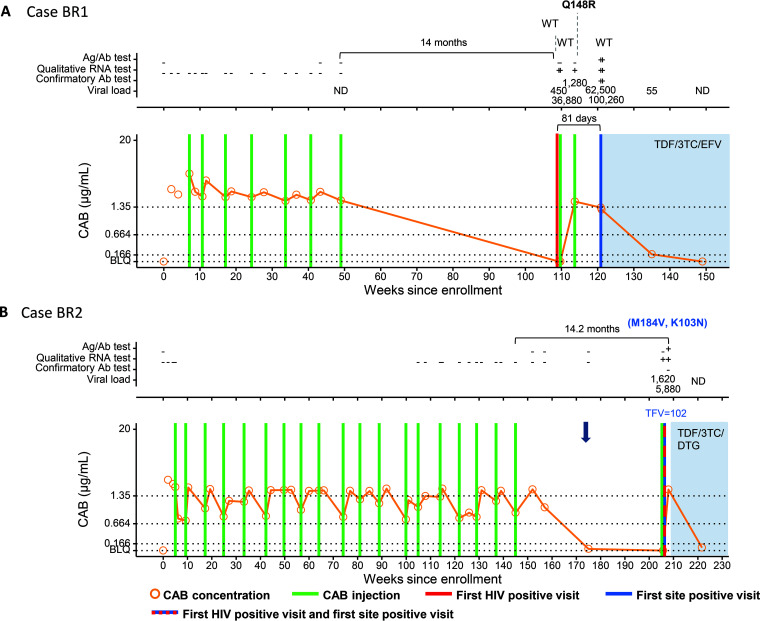
HPTN 083 demonstrated that injectable cabotegravir (CAB) was superior to oral tenofovir disoproxil fumarate-emtricitabine (TDF-FTC) for HIV prevention in cisgender men and transgender women who have sex with men. We previously analyzed 58 infections in the blinded phase of HPTN 083 (16 in the CAB arm and 42 in the TDF-FTC arm). This report describes 52 additional infections that occurred up to 1 year after study unblinding (18 in the CAB arm and 34 in the TDF-FTC arm). Retrospective testing included HIV testing, viral load testing, quantification of study drug concentrations, and drug resistance testing. The new CAB arm infections included 7 with CAB administration within 6 months of the first HIV-positive visit (2 with on-time injections, 3 with ≥1 delayed injection, and 2 who restarted CAB) and 11 with no recent CAB administration. Three cases had integrase strand transfer inhibitor (INSTI) resistance (2 with on-time injections and 1 who restarted CAB). Among 34 CAB infections analyzed to date, diagnosis delays and INSTI resistance were significantly more common in infections with CAB administration within 6 months of the first HIV-positive visit. This report further characterizes HIV infections in persons receiving CAB preexposure prophylaxis and helps define the impact of CAB on the detection of infection and the emergence of INSTI resistance.
Keywords: HIV; HPTN 083; TDF-FTC; cabotegravir; injectable; long-acting; men who have sex with men; preexposure prophylaxis; prevention.
Conflict of interest statement
The authors declare a conflict of interest. None of the authors has a commercial or other association that might pose a conflict of interest, with the following exceptions: R.J.L. has served on scientific advisory boards for Gilead and Merck, and has received honoraria from Roche and Janssen. J.F.R. is an employee and stockholder of Gilead Sciences. M.St.C. and A.R.R. are employees of ViiV Healthcare. S.L.F. is an employee of GlaxoSmithKline.
Figures
References
-
- Landovitz RJ, Donnell D, Clement ME, Hanscom B, Cottle L, Coelho L, Cabello R, Chariyalertsak S, Dunne EF, Frank I, Gallardo-Cartagena JA, Gaur AH, Gonzales P, Tran HV, Hinojosa JC, Kallas EG, Kelley CF, Losso MH, Madruga JV, Middelkoop K, Phanuphak N, Santos B, Sued O, Valencia Huamani J, Overton ET, Swaminathan S, Del Rio C, Gulick RM, Richardson P, Sullivan P, Piwowar-Manning E, Marzinke M, Hendrix C, Li M, Wang Z, Marrazzo J, Daar E, Asmelash A, Brown TT, Anderson P, Eshleman SH, Bryan M, Blanchette C, Lucas J, Psaros C, Safren S, Sugarman J, Scott H, Eron JJ, Fields SD, et al. 2021. Cabotegravir for HIV prevention in cisgender men and transgender women. N Engl J Med 385:595–608. doi: 10.1056/NEJMoa2101016. - DOI - PMC - PubMed
-
- Delany-Moretlwe S, Hughes JP, Bock P, Ouma SG, Hunidzarira P, Kalonji D, Kayange N, Makhema J, Mandima P, Mathew C, Spooner E, Mpendo J, Mukwekwerere P, Mgodi N, Ntege PN, Nair G, Nakabiito C, Nuwagaba-Biribonwoha H, Panchia R, Singh N, Siziba B, Farrior J, Rose S, Anderson PL, Eshleman SH, Marzinke MA, Hendrix CW, Beigel-Orme S, Hosek S, Tolley E, Sista N, Adeyeye A, Rooney JF, Rinehart A, Spreen WR, Smith K, Hanscom B, Cohen MS, Hosseinipour MC, HPTN 084 Study Group . 2022. Cabotegravir for the prevention of HIV-1 in women: results from HPTN 084, a phase 3, randomised clinical trial. Lancet 399:1779–1789. doi: 10.1016/S0140-6736(22)00538-4. - DOI - PMC - PubMed
-
- Marzinke MA, Grinsztejn B, Fogel JM, Piwowar-Manning E, Li M, Weng L, McCauley M, Cummings V, Ahmed S, Haines CD, Bushman LR, Petropoulos C, Persaud D, Adeyeye A, Kofron R, Rinehart A, St Clair M, Rooney JF, Pryluka D, Coelho L, Gaur A, Middelkoop K, Phanuphak N, Cohen MS, Hendrix CW, Anderson P, Hanscom B, Donnell D, Landovitz RJ, Eshleman SH. 2021. Characterization of human immunodeficiency virus (HIV) infection in cisgender men and transgender women who have sex with men receiving injectable cabotegravir for HIV prevention: HPTN 083. J Infect Dis 224:1581–1592. doi: 10.1093/infdis/jiab152. - DOI - PMC - PubMed
-
- Eshleman SH, Fogel JM, Halvas EK, Piwowar-Manning E, Marzinke MA, Kofron R, Wang Z, Mellors J, McCauley M, Rinehart AR, St Clair M, Adeyeye A, Hinojosa JC, Cabello R, Middelkoop K, Hanscom B, Cohen MS, Grinsztejn B, Landovitz RJ, HPTN 083 Study Team . 2022. HIV RNA screening reduces integrase strand transfer inhibitor resistance risk in persons receiving long-acting cabotegravir for HIV prevention. J Infect Dis 226:2170–2180. doi: 10.1093/infdis/jiac415. - DOI - PMC - PubMed
-
- Han K, Baker M, Lovern M, Paul P, Xiong Y, Patel P, Moore KP, Seal CS, Cutrell AG, D’Amico RD, Benn PD, Landovitz RJ, Marzinke MA, Spreen WR, Ford SL. 2022. Population pharmacokinetics of cabotegravir following administration of oral tablet and long-acting intramuscular injection in adult HIV-1-infected and uninfected subjects. Br J Clin Pharmacol 88:4607–4622. doi: 10.1111/bcp.15439. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
