

Risk and Timing of De Novo Sepsis in Critically Ill Children after Acute Kidney Injury
- PMID: 36996298
- PMCID: PMC10103342
- DOI: 10.34067/KID.0005082022
Risk and Timing of De Novo Sepsis in Critically Ill Children after Acute Kidney Injury
Abstract
Key Points:
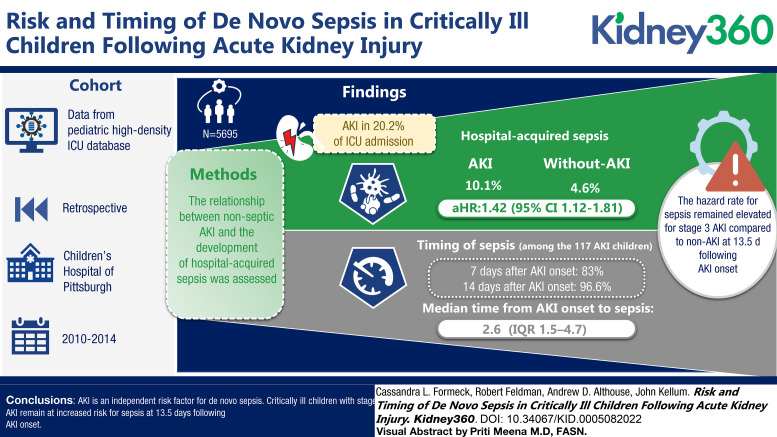
Critically ill children who developed AKI have a 42% increase in the probability of developing subsequent hospital-acquired sepsis when compared with children without AKI.
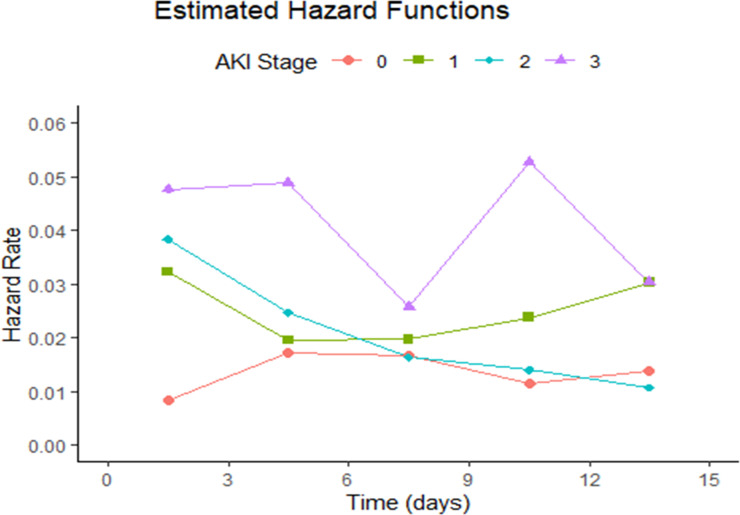
When evaluating risk of sepsis over time, children with stage 3 AKI remain at increased risk for sepsis for at least 2 weeks after AKI onset.
Medical providers should monitor for signs of sepsis after AKI and limit exposures that may increase the risk for infection.
Background: AKI is common among critically ill children and is associated with an increased risk for de novo infection; however, little is known about the epidemiology and temporal relationship between AKI and AKI-associated infection in this cohort.
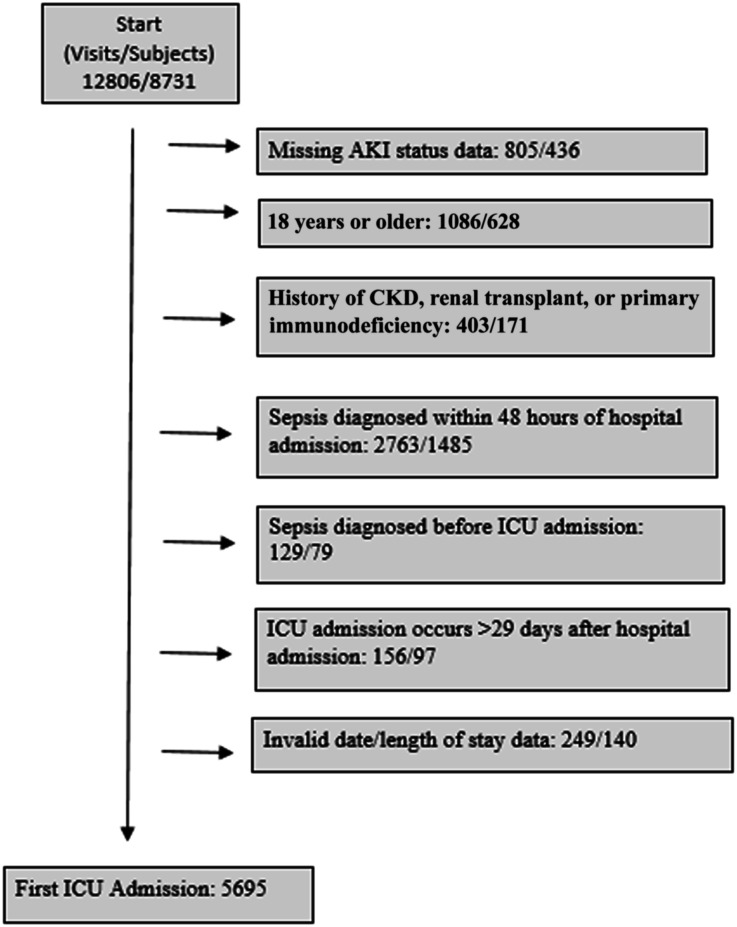
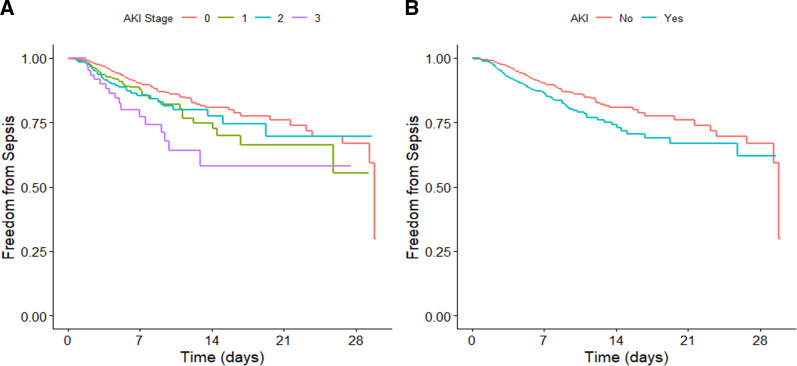
Methods: We conducted a single-center retrospective cohort study of children admitted to the pediatric and cardiac intensive care units (ICUs) at a tertiary pediatric care center. The relationship between nonseptic AKI and the development of hospital-acquired sepsis was assessed using Cox proportional hazards models using AKI as a time-varying covariate.
Results: Among the 5695 children included in this study, AKI occurred in 20.2% from ICU admission through 30 days. Hospital-acquired sepsis occurred twice as often among children with AKI compared with those without AKI (10.1% versus 4.6%) with an adjusted hazard ratio of 1.42 (95% confidence interval, 1.12 to 1.81). Among the 117 children who developed sepsis after AKI, 80.3% developed sepsis within 7 days and 96.6% within 14 days of AKI onset, with a median time from AKI onset to sepsis of 2.6 days (interquartile range, 1.5–4.7). When assessing change in risk over time, the hazard rate for sepsis remained elevated for children with stage 3 AKI compared with children without AKI at 13.5 days after AKI onset, after which the estimation of hazard rates was limited by the number of children remaining in the hospital.
Conclusions: AKI is an independent risk factor for de novo sepsis. Critically ill children with stage 3 AKI remain at increased risk for sepsis at 13.5 days after AKI onset.
Conflict of interest statement
J.A. Kellum reports the following: Employer: Spectral Medical; University of Pittsburgh School of Medicine; University of Pittsburgh Medical Center (on leave); Consultancy: AM Pharma, Astellas, Astute Medical, Baxter, bioMerieux, Cytosorbents, Grifols, Klotho, Mallinckrodt, NxStage, PhotoPhage, Potrero, RenalSense; Ownership Interest: J3RM, Klotho, Photophage, Spectral Medical; Research Funding: Astute Medical, Astellas, Baxter, bioMerieux, Grifols, Cytosorbents, Atox Bio, Astellas, Bioporto, RenalSense; Patents or Royalties: Astute Medical, Cytosorbents, J3RM, Klotho, Photophage; and Advisory or Leadership Role: Editor: Critical Care Clinics of North America; Editorial Boards: Nephrology Dialysis Transplantation; Critical Care; Critical Care Medicine; Blood Purification. All remaining authors have nothing to disclose.
Figures
Comment in
-
Sepsis and AKI: A Two-Way Street.Kidney360. 2023 Mar 1;4(3):289-290. doi: 10.34067/KID.0000000000000106. Kidney360. 2023. PMID: 36996291 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
